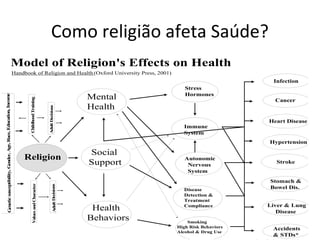
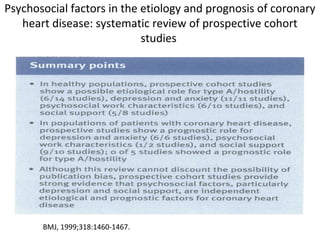
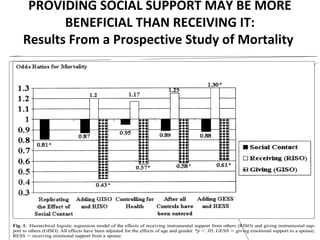
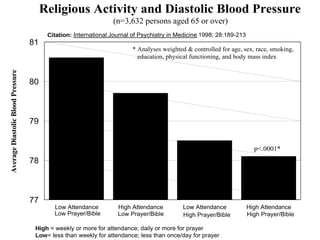
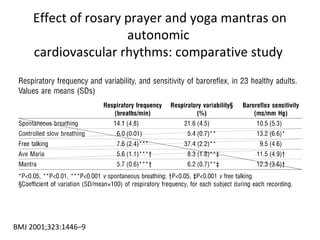
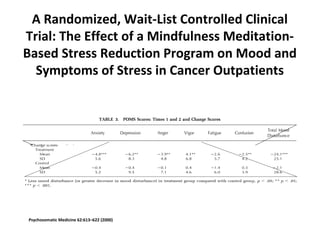
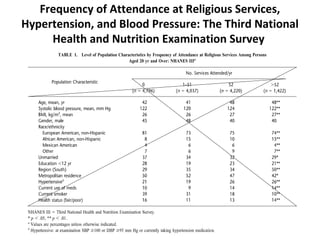
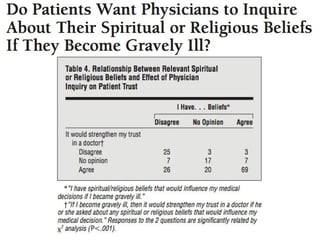
The document discusses applying spirituality clinically from two perspectives in dialogue. It begins with a declaration of conflict of interest as the author has religious faith. It then discusses how to define and measure spirituality versus religion. Several studies are summarized that examine relationships between religion, spirituality and health outcomes like depression, anxiety, blood pressure and mortality. The author suggests a respectful approach to discussing spirituality with patients and hopes to stimulate interest in further studying this topic to benefit primary care in Brazil.