Downloaded 42 times


![1) Age younger than 40yrs at disease onset
2) Claudication of the extremities
3) Decreased pulsation of one or both brachial arteries
4) Difference of at least 10 mm Hg in systolic blood
pressure between arms
5) Bruit over 1 or both subclavian arteries or the
abdominal aorta
6) Arteriographic narrowing or occlusion of the entire
aorta, its primary branches, or large arteries in the
upper or lower extremities that is not due to
arteriosclerosis, fibromuscular dysplasia, or other
causes
The presence of any 3 or more criteria yields a
sensitivity of 90.5% and a specificity of 97.8%.[20]](https://image.slidesharecdn.com/takayasuarteritiscasepresentation-141029021251-conversion-gate02/85/Takayasu-arteritis-case-presentation-20-320.jpg)
![1) Age of 40 years or younger at disease onset
2) Claudication of the extremities
3) Decreased pulsation of 1 or both brachial arteries
4) Difference of at least 10 mm Hg in systolic blood
pressure between arms
5) Bruit over 1 or both subclavian arteries or the
abdominal aorta
6) Arteriographic narrowing or occlusion of the entire
aorta, its primary branches, or large arteries in the
upper or lower extremities that is not due to
arteriosclerosis, fibromuscular dysplasia, or other
causes
The presence of any 3 or more criteria yields a
sensitivity of 90.5% and a specificity of 97.8%.[20]](https://image.slidesharecdn.com/takayasuarteritiscasepresentation-141029021251-conversion-gate02/85/Takayasu-arteritis-case-presentation-27-320.jpg)
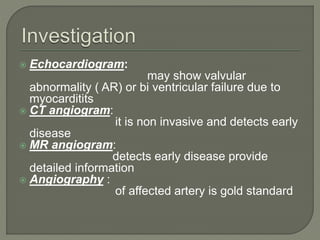


This document describes the case of a 22-year old female patient who presented with 1 month of left upper limb pain. On examination, she was found to have absent left radial pulse and diminished left brachial and ulnar pulses. Testing showed elevated ESR and imaging found stenosis of the left subclavian artery. She was diagnosed with Takayasu's arteritis. She was treated with steroids and methotrexate, which improved her symptoms, and later underwent stenting of the left subclavian artery. Takayasu's arteritis is an inflammatory condition involving medium and large arteries that commonly affects younger women and can cause limb ischemia.













































































