The Immune Response
Immunity: “Free from burden”. Ability of an organism to recognize and defend itself against specific pathogens or antigens.
Immune Response: Third line of defense. Involves production of antibodies and generation of specialized lymphocytes against specific antigens.
Antigen: Molecules from a pathogen or foreign organism that provoke a specific immune response
immunity, types,Innate immunity and Adaptive Immunity, primary and secondary immune response, structure and functions of antibodies, immunoglobulins, hypergammaglobulinemia, multiple myeloma, bence jones protein, electrophoretic pattern of multiple myeloma.
The Immune Response
Immunity: “Free from burden”. Ability of an organism to recognize and defend itself against specific pathogens or antigens.
Immune Response: Third line of defense. Involves production of antibodies and generation of specialized lymphocytes against specific antigens.
Antigen: Molecules from a pathogen or foreign organism that provoke a specific immune response
immunity, types,Innate immunity and Adaptive Immunity, primary and secondary immune response, structure and functions of antibodies, immunoglobulins, hypergammaglobulinemia, multiple myeloma, bence jones protein, electrophoretic pattern of multiple myeloma.
The organism possesses powerful mechanism to avoid immune auto aggression, The acquired ability of the immune system to avoid responsiveness to self antigens is defined as ‘ tolerance’ It is obtained by the cooperative efforts of central and peripheral mechanisms, which allow a rapid and efficient removal of pathogens ( Virus and Bacteria ) in the absence of self-recognition, It is a dysfunction of the immune system. The immune system protects you from disease and infection. Sometimes, though, the immune system can produce autoantibodies that attack healthy cells, tissues, and organs. This can lead to autoimmune disease.Autoimmune diseases can affect any part of the body
This is the process by which individual’s immune system becomes fortified against an infectious agents (immunogen) to a subsequent encounter naturally or , also achieved by vaccination.
An exaggerated immune response to innocuous antigens (harmless foreign substance) in an individual upon reexposure. Also known as Hypersensitivity or Allergic reactions.
Tolerance and Autoimmunity By Dr. Kanury Rao.pptxDr.Kanury Rao
The term ‘immune tolerance’ indicates the lack of response of the immune mechanism to its own antigens. The autoimmunity is caused by the breakdown of immunity tolerance. Dr. Kanury Rao is analyzing the causes and preventions of these diseases
Indian Dental Academy: will be one of the most relevant and exciting training center with best faculty and flexible training programs for dental professionals who wish to advance in their dental practice,Offers certified courses in Dental implants,Orthodontics,Endodontics,Cosmetic Dentistry, Prosthetic Dentistry, Periodontics and General Dentistry.
2. INTRODUCTION
My storybeginsin 2003.
In2003 Ivisited my gynaecologist formy regular yearly check-up.There were some
concerns as Iwas seriously under weight.Aftermycheck-up Iwas informed thatIhadmild
Endometriosis as well as several fibroidsin myuterus. Thegynaecologist bookedmetohave
itremoved. All wentwell withtheoperation,butafterwards Iwas notgettingbetter. I
startedgaining drastic weight.Twoweeks afterthe operationI faintedat workandwas
rushedback tomygynaecologist andI wasadmitted tohospitalstraight away.Atthisstage
itwas established thatmy kidneyswere onlyfunctioning at10%capacity and thatIhada
severe kidney infection. Iwas treatedanddischarged from hospitalwithanti-biotic. Weight
gain wasa serious problem afterthat. I gained20kgin less than2 months. InoticedthatI
periodically feltfeverish. My hair fell outin clumps andIbecame verysensitive tosunlight.I
complained aboutthesymptoms tomyG.Ponseveral occasions andwas prescribed
painkillers. He performed several bloodtestsandputall mysymptoms downtoanunder
active thyroid and rheumatoid arthritis. My bloodpressurehad sky-rocketedas well as my
cholesterol levels. Throughall this, Ihave triedto lose weightwithno success.
Eventually in January 2012thefeverish aches and pains andweightgain forced me tochange
G.P’s.Thenew G.Pperformedseveral bloodtests,butwasunable tomake anydiagnosis and
decidedit wastime for me tovisit aPhysician. On2 April2012 thePhysician diagnosed me
withSystemic LupusErythmatosis. Afterseveral more tests,itwas confirmed thatIam
living withLupusNephritis. Presently weare experimenting withdifferent medications
anddiets tofindthe bestwaytotreat it.
DEFINITION – WHATIS LUPUS
“Lupus” means “wolf” in Latin. This is an indication of the rough appearance Lupus gives to
the skin. In Lupus, the body's immune system does not work as it should. Lupus is an
inflammatory and autoimmune disease of the connective tissue. It is classified as an
autoimmune disease, since the body attacks itself. It is a chronic autoimmune disease that
causes the immune systemto attack tissue and organs including the joints, kidneys, heart,
lungs, brain blood or skin.
SLE differs from HIV AIDS as HIV destroys the body’s immune system, but SLE is a person’s
immune systemdestroying the connective systemin his or her own body.
3. Inmy case, itis attacking mainly my kidneysas well as joints,heart andnervous system.
A healthy immune systemproduces substances called antibodies that help fight and destroy
viruses, bacteria, and other foreign substances that invade the body. Antibodies are protein
molecules produced by a substance called antigens. An antigen is any substance capable of
exciting the immune systemand provoking an immune response. Most antigens are large,
complex molecules such as proteins and carbohydrates that are not normally present in our
bodies. Haptens are smaller molecules that may become antigens by combining with larger
molecules. As far as our immune systemis concerned, antigens are “nonself”. An almost
limitless variety of substances can act as antigens, including virtually all foreign proteins,
nucleic acids, large carbohydrates and some lipids. Of these, proteins are the strongest
antigen. Our own cells are richly studded with a variety of protein molecules, called “self-
antigens”. Somehow, as our immune systemdevelops, it takes an inventory of all these
proteins, so that, thereafter, they are recognised as “self”. In healthy individuals these ‘self-
antigens” do not trigger an immune response, but it seems to trigger a response in people
with Lupus.
Antibodies are also referred to as immunoglobulins or Igs. Igs constitute the gamma globulin
part of blood proteins. Antibodies are soluble proteins secreted by activated B cells or by
their plasma-cell offspring in response to an antigen, and they are capable of binding
specifically with that antigen. Antibodies are made by white blood cells, lymphocytes, in the
spleen and in lymph nodes. A particular group os lymphocytes, or B-cells, produce plasma
cells which in turn make antibodies when exposed to an antigen.
There are 5 main classes of immunoglobulins:
4. IgG – 75% - neutralizes viruses and toxins
IgA – Protects the surface of the body
IgM – Assists in the consumption of bacteria
IgE – Is responsible for allergic reactions
IgD – Important in activation of B-cells
Regardless of its class, antibodies have a basic structure consisting of four amino acid
(polypeptide) chains linked together by disulfide (sulfer to sulfer) bonds. Two of the four
chains are identical and contain approximately 400 amino acids each, these are ‘heavy
chains’. The other two chains, the ‘light chains’ are also identical to each other but are only
about half as long. When the four chains are combined, the antibody molecule formed has
two identical halves, each consisting of a ‘heavy’ and a ‘light’ chain and the molecule as a
whole is “T” of “Y” shaped. Each of the chains forming an antibody has a variable – V region
at one end and a much larger constant –C region at the other end. Antibodies responding to
different antigens has very different variable regions, but the constant regions stay the
same or nearly so. The variable regions of the heavy and light chains in each arm combine
their efforts to form and antigen-binding site uniquely shaped to “fit” its specific antigen.
Thus each antibody has two antigen binding regions.
When the immune systemfirst comes into contact with an antigen it is called the primary
response and the antibodies are usually found in the blood stream after approximately 1
week. If a person comes into contact with the same antigen for a second time, antibodies
will appear in the blood stream much earlier, reaching higher levels and are maintained for
a longer time. This response is called secondary response and is an important part of the
body’s defence mechanism. This is why we only succumb to some diseases once. After initial
infection antibodies will remain in the blood for many years and can wipe-out infections
before they can take hold.
Antibodies inactivate antigens in a number of ways: by complement fixation, neutralization,
agglutination, and precipitation.
Neutralization occurs when antibodies bind to specific sites on bacterial exotoxins (toxic
chemicals secreted by bacteria) or viruses that can cause cell injury. In this way, they block
the harmful effects of exotoxin or virus.
Because antibodies have more than one antigen-binding site, they can bind to more than
one antigen at a time, consequently, antigen-antibody complexes can be cross-linked into
large lattices. When the cross-linking involves cell-bound antigens, the process causes
clumping of the foreign cells, a process called agglutination.
The antibody can also cause a bacterium to burst open.
Phagocytosis can be used by the antibody to engulf the foreign organism.
It can also prevent the organism from attaching itself to, and damaging, body cells.
5. Another form of defence by antibodies against infection is cell-mediated immunity. T-
lymphocytes, or white blood cells, occur in lymph fluid, lymph tissue as well as blood. When
they encounter an antigen, they are stimulated to set into motion mechanisms aimed at
destroying the invading organism – including the stimulation of the mother defence system
called compliment. Inflammatory response starts with T-lymphocytes.
Interferon is another system in the body’s defence mechanism which is activated by virus
infections. Interferon has a generalized effect on all types of viruses and so, if it is induced
by one type of virus, it can also inhibit the multiplication of other, un-related viruses to
which the body is normally susceptible.
Normally, the immune system helps protect the body from infection or harmful substances.
But in patients with an autoimmune disease, the immune system cannot tell the difference
between harmful substances and healthy ones. As a result, the immune system attacks
otherwise healthy cells and tissue
In Lupus, the immune systemproduces antibodies against the body's healthy cells and
tissues. These antibodies, called autoantibodies ("auto" meaning self), contribute to the
inflammation of various parts of the body, causing damage and altering the function of
target organs and tissues. In addition, some autoantibodies join with substances from the
body's own cells or tissues to form molecules called immune complexes. A build-up of these
immune complexes in the body also contributes to inflammation and tissue injury in people
with lupus. Researchers do not yet understand all of the factors that cause inflammation
and tissue damage in Lupus, and this is an active area of research. In lupus the immune
system loses its ability to tell the difference between foreign substances and its own cells
and tissues. The immune system then makes antibodies directed against “self”.
One longstanding proposed mechanism for the development of autoantibodies involves a
defect in apoptosis that causes increased cell death and a disturbance in immune tolerance.
The redistribution of cellular antigens during necrosis or apoptosis leads to a cell-surface
display of plasma and nuclear antigens in the form of nucleosomes. Subsequently, intolerant
lymphocytes begin targeting normally protected intracellular antigens. There seems to be
disruptions in lymphocyte signalling, interferon response, clearance of complement and
immune complexes, apoptosis, and DNA methylation.
Many clinical manifestations of SLE are mediated via circulating immune complexes in
various tissues or the direct effects of antibodies to cell surface components. Immune
complexes form in the microvasculature, leading to complement activation and
inflammation. Moreover, antibody-antigen complexes deposit on the basement membranes
of skin and kidneys. In active SLE, this process has been confirmed by demonstration of
6. complexes of nuclear antigens such as DNA, immunoglobulins, and complement proteins at
these sites.
Serum antinuclear antibodies (ANAs) are found in nearly all individuals with active SLE.
Antibodies to native double-stranded DNA (dsDNA) are relatively specific for the diagnosis
of SLE. Whether polyclonal B-cell activation or a response to specific antigens exists is
unclear, but much of the pathology involves B cells, T cells, and dendritic cells. Cytotoxic T
cells and suppressor T cells, which would normally down-regulate immune responses, are
decreased. The generation of polyclonal T-cell cytolytic activity is impaired. Helper (CD4) T
cells are increased. A lack of immune tolerance is observed in SLE patients. Recent reports
pointing to important roles of interferon alpha, transcription factors, and signalling
variations also point to a central role for neutrophils.
CAUSES
The cause of Lupus is not fully known. Certain factors have so far been identified as possible
causes. These factors range from Ultraviolet rays, stress, shock, childbirth, fatigue, viral or
7. bacterial infections, chemicals and drugs as well as genetic, racial, hormonal and
environmental factors.
Lupus is much more common in women than in men. It may occur at any age, but appears
most often in people between the ages of 10 and 50 years of age. Women of colour are
affected more than Caucasian women. It also appears that Lupus occurs more in women in
their 30’s than at any other age.
Studies have been done to get more clarity on what is known about the mechanisms of SLE
disease and genetic associations. It has been found that at least 35 genes are known to
increase the risk of SLE. A genetic predisposition is supported by the 40% concordance
among monozygotic twins. If a mother has SLE, her daughter's risk of developing the disease
has been estimated at 1:40 and her son's risk is 1:250.
Human leukocyte antigens (HLA) - HLA-A1, B8, and DR3 are more common in persons with
SLE than in the general population. The presence of the null complement alleles and
congenital deficiencies of complement, especially C4, C2, are also associated with an
increased risk of SLE.
Some studies have investigated the role of infectious aetiologies that may also maintain
autoimmunity. Patients with SLE have higher titers of antibodies to Epstein-Barr virus (EBV),
have increased circulating EBV viral loads, and make antibodies to retroviruses, including to
protein regions homologous to nuclear antigens. Viruses may stimulate specific cells in the
immune network. Chronic infections may induce anti-DNA antibodies or even Lupus-like
symptoms, and acute Lupus flares often follow bacterial infections.
Environmental and exposure-related causes of SLE are less clear. Silica dust and cigarette
smoking may increase the risk of developing SLE. Administration of oestrogen to
postmenopausal women appears to increase the risk of developing SLE. Breastfeeding is
associated with a decreased risk of developing SLE.
The results of one study suggest that low vitamin D levels increase autoantibody production
in healthy individuals; vitamin D deficiency was also linked to B-cell hyperactivity and
interferon-alpha activity in patients with SLE.
Thecause tomyLupusseems tobe fromthe operationI hadin2003 totreatEndometriosis
andfibroids andthesubsequentkidney infection. Atthetime Iwas also given oestrogen
replacements bymygynaecologist for ahormonal imbalance, which may have beena
contributingfactor.
SYMPTOMS
People with Lupus often have features that are not specific to Lupus. Symptoms may vary
substantially from person to person. Usually when a person presents with four or more of
8. the symptoms listed below and the doctor cannot find any other reason for them, he will
test for Lupus:
Painful or swollen joints and muscle pain
High blood pressure
Depression
Unexplained fever
Red rashes, most commonly on the face.
Chest pain upon deep breathing (pleurisy)
Unusual loss of hair
Heartburn or stomach pain
Pale or purple fingers or toes from cold or stress (Raynaud's phenomenon)
Sensitivity to the sun
Swelling (oedema) in legs or around eyes
Swollen glands
Extreme fatigue
Unexplained weight loss or gain
High cholesterol levels
Mouth sores lasting from a few days to more than a month
Abnormal blood tests – low white blood cells or platelet counts
Pregnant women who have unexplained miscarriages
unexplained hair loss
In some people with Lupus, only one systemof the body such as the skin or joints is
affected. Other people experience symptoms in many parts of their body. Just how seriously
a body system is affected also varies from person to person. Most commonly, joints and
muscles are affected, causing arthritis and muscle pain. Skin rashes are quite common.
The following systems in the body can also be affected by SLE:
9. Kidneys: Inflammation of the kidneys (nephritis) can impair their ability to get rid of waste
products and other toxins from the body effectively. Because the kidneys are so important
to overall health, Lupus affecting the kidneys generally requires intensive drug treatment to
prevent permanent damage. There is usually no pain associated with kidney involvement,
although some patients may notice that their ankles swell or they retain water throughout
the body. Most often the only indication of kidney disease is an abnormal urine or blood
test.
Lungs: Some people with Lupus develop pleuritis, an inflammation of the lining of the chest
cavity that causes chest pain, particularly with breathing. Patients with Lupus also may get
pneumonia.
Lupus and Lung Problems
The tissue surrounding the lungs becomes inflamed in abouta third of people with lupus.This may lead to painful
breathing,or chestpain,or it may not cause any symptoms atall.Sometimes lupus causes chestpain thatis not
related to the lungs or the heart. Instead,the pain comes from an inflamed chestmuscle or rib joint. Any chest
pain should be promptlyevaluated by a doctor.
10. Central nervous system: In some patients, Lupus affects the brain or central nervous
system. This can cause headaches, dizziness, memory disturbances, vision problems, stroke,
seizures, or changes in behaviour.
Blood vessels: Blood vessels may become inflamed (vasculitis), affecting the way blood
circulates through the body. The inflammation may be mild and may not require treatment
or may be severe and require immediate attention.
Blood: Lupus sufferers may develop anaemia, leucopoenia (a decreased number of white
blood cells), or a decrease in the number of platelets (thrombocytopenia). Some people
with Lupus may have abnormalities that cause an increased risk for blood clots.
Heart: In some Lupus patients, inflammation can occur in the heart itself (myocarditis and
endocarditis) or the membrane that surrounds it
(pericarditis), causing chest pains or other
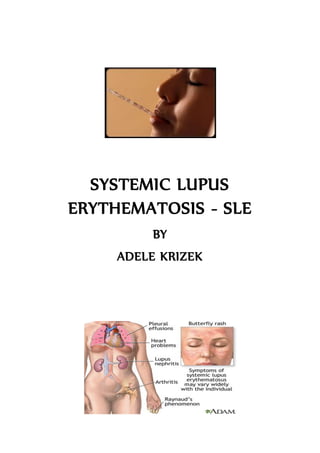
symptoms. Lupus can also increase the risk of
atherosclerosis.
11. “Butterfly” shapedrash over the cheeks
Lupus cancause multipleorgansto be inflamedincluding:kidneys,liningtissueofthe heart and
lungsandthe brain
My symptomsincludes painful andswollen joints, muscle pain, arthritic pain,permanent
unexplained fever, chestpain, unusual hair loss,swelling in legs,hands,arms around the
12. eyes, extreme fatigue,impaired vision, depression, dizziness, headaches, unexplained
weightgain, highbloodpressure andhighcholesterol.
TYPES OF LUPUS
There are four types of lupus:
Discoid Lupus erythematosis affects the skin. Discoid Lupus is also known as
coetaneous Lupus.
Drug-induced Lupus erythematosis occurs as a side effect of some drugs, such as beta
blockers, which are commonly used to treat heart disease and hypertension. Hormone
replacements such as oestrogen, has also been identified as a possible cause.
Neonatal lupus erythematosis is a rare form of Lupus in newborn babies whose
mothers have lupus, which can cause problems at birth or a serious heart defect in
rare cases.
Neonatal Lupus
Most babies born to women with lupus are entirelyhealthy. But in rare cases,the newborn of a mom with lupus
may have neonatal lupus.This condition can cause a skin rash,anemia,or liver problems.The symptoms usually
go away after a few months and don't cause permanentdamage.However,some babies with neonatal lupus can
be born with a serious heartproblem
Systemic Lupus Erythematosis causes inflammation in multiple organs and body
systems eg: Lupus Nephritis is Lupus where the kidneys are inflamed.
14. DIAGNOSIS –TESTS PERFORMED
Diagnosing Lupus
Diagnosing lupus can be tricky. The disease can mimic other conditions,and it often takes a different course in
different people.Many people have it for years before developing tell-tale symptoms.Although there is no one
test for lupus,certain proteins usuallyshow up in a patient's blood.A blood test for antinuclear antibodies (ANAs)
can provide a critical clue.Other lab tests may check cell counts,kidney function, and clotting time. A tissue
biopsyof an involved organ such as the skin or kidneys s ometimes helps with diagnosis.
A LFA survey of its members suggests that more than half of those afflicted with Lupus
suffered at least four years, and saw three or more doctors before obtaining a correct
diagnosis of Lupus.
Nearly half of the survey participants (49%) received their diagnosis of Lupus after being
examined by a rheumatologist, a medical specialist who treats diseases of the connective
tissue.
4 out of 5 Lupus patients are treated by three or more doctors, and take six or more
medications to treat symptoms of the disease.
To be diagnosed with Lupus, a person must have at least 4 of the 11 typical signs of the
disease.
A doctor will perform a physical exam which includes listening to your chest with a
stethoscope. An abnormal sound called a ‘heart fiction rub’ or ‘pleural friction rub’ may be
heard. A nervous system exam may also be done.
No single laboratory test can determine whether a person has Lupus.
The anti-nuclear antibody (ANA) test is used as a screening test for lupus. We know that 95
percent of people with lupus have a positive ANA. Therefore, if a person has symptoms of
systemic lupus but their ANA test is negative, that's generally regarded as pretty good
evidence against lupus being the explanation for the symptoms they are having.
On the other hand, if the ANA test comes back positive, that IS NOT proof that the person
has Lupus. The positive ANA is only an indicator; it is not diagnostic. A positive ANA can be
15. found in a number of illnesses and conditions. In fact, many people may have positive Lupus
tests-particularly the anti-nuclear antibody test-and yet they do NOT have the disease.
All lab tests have normal values. If a test result comes back and the value is at the upper
limit of normal, this is often referred to as being on the border or borderline. These results
are often very difficult to interpret; and the assessment of its importance is dependent on
meeting other criterion.
A variety of laboratory tests are used to detect physical changes or conditions in the body
that can occur with Lupus. Each test result adds more information to the body of evidence
that a doctor uses to determine if a person has Lupus. However, Lupus cannot be diagnosed
solely on lab work. A lupus diagnosis is made by a careful review of the following:
• a person’s current symptoms,
• laboratory test results for other antibodies, especially anti-double-strand DNA
antibodies,
• medical history, and
• the medical history of close family members (grandparents, parents, brothers and
sisters, aunts, uncles, cousins).
Blood tests performed include:
The antinuclear antibody panel is a blood test that looks at antinuclear antibodies (ANA).
Antinuclear antibodies are substances produced by the immune system that attack the
body’s own issues.
Usually there is no detectable ANA in the blood and the test will be negative.
ANA is reported as a “titer”. Low titers are in the range of 1:40 to 1:60. A positive ANA is
much more significant if you also have antibodies against the double-stranded form of DNA.
ANA does not confirm a diagnosis of SLE, but a lack of ANA makes SLE diagnosis less likely.
The Compliment is a blood test that measures the activity of certain proteins in the liquid
portion of the blood. The Compliment systemis a group of proteins that move freely
through the bloodstream. The proteins work with the immune system and play a role in the
development of inflammation. There are 9 major Complement proteins and they are
numbered C1-C9. Total Compliment activity (CH50, CH100) looks at the overall activity of
the Complement System. The Complement test is performed after other more specific tests
for a suspected disease are performed. C3 and C4 are the most commonly measured
Complement components. People with active SLE may have lower-than-normal levels of the
Complement proteins C3 and C4.
The BUN test is a blood test and stands for Blood Urea Nitrogen. Urea Nitrogen is what
forms when protein breaks down. The BUN test is done to measure the amount of urea
nitrogen in the blood.
Many drugs affect BUN levels. Drugs that can increase BUN levels include Aspirin, Bacitracin,
Chloral Hydrate, Furosemide, Methicillin, Penicillamine and Triamterene. Drigs that can
decrease BUN measurements include Chloramphenicol and Streptomycin.
16. A normal BUN result is generally 6-20mg/dL. The BUN test is usually done to check kidney
function in a person who has SLE.
Other tests that are used to diagnose SLE may include:
CBC
Chest X-Ray
Kidney biopsy
Urinalysis
Creatinine
Urinalysis is the physical, chemical, and microscopic examination of urine. It involves a
number of tests to detect and measure various compounds that pass through the urine.
The sample of urine is sent to a lab, where it examined for the following:
Physical colour and appearance:
What does the urine look like to the naked eye?
Is it clear or cloudy?
Is it pale or dark yellow or another colour?
The urine specific gravity test reveals how concentrated or dilute the urine is.
Microscopic appearance:
The urine sample is examined under a microscope to look at cells, urine crystals,
mucus, and other substances in the sample, and to identify any bacteria or other
germs that might be present.
Chemical appearance:
A special stick ("dipstick") tests for various substances in the urine. The stick
contains little pads of chemicals that change color when they come in contact with
the substances of interest.
Creatinine is a breakdown product of creatine, which is an important part of muscle. A
blood sample is needed. Creatinine can also be measured with a urine test. The test is done
to see how well your kidneys work. Creatinine is removed from the body entirely by the
kidneys. If kidney function is abnormal, creatinine levels will increase in the blood (because
less creatinine is released through your urine).
Creatinine levels also vary according to a person's size and muscle mass.
A measurement of the serum creatinine level is often used to evaluate kidney function.
Urine creatinine levels can be used as a screening test to evaluate kidney function, or can be
part of the creatinine clearance test.
17. Tests thathavebeen performed onme tomake afull diagnosis were: Antinuclear Panel,
BUN,Compliment test,Urine Analysis, andCreatinine. Inaddition Ihave also goneforX-
rays onmy chestand joints, had sonar onmy kidneysas well as myheart andhadtoperform
an EffortECG.
CONVENTIONAL TREATMENT
There is no cure for SLE. The goal of treatment is to control symptoms. The correct
medication and dosage is established through trial and error by experimenting with
different drugs and dosages until the symptoms improve.
Mild SLE may be treated with:
Non-steroidal anti-inflammatory medications (NSAIDs) treat arthritis and pleurisy
Corticosteroid creams to treat skin rashes
An anti-malaria drug (hydroxychloroquine) and low-dose corticosteroids for skin
and arthritis symptoms
A person with Lupus should wear protective clothing, sunglasses, and sunscreen when going
out in the sun.
Severe or life-threatening symptoms, such as haemolyticanaemia, extensive heart or lung
involvement, kidney disease, or central nervous system involvement, often require more
aggressive treatment by doctor specialists.
Treatment for more severe SLE may include:
High-dose corticosteroids or medications to decrease the immune system response
Cytotoxic drugs (drugs that block cell growth) if you do not get better with
corticosteroids, or whose symptoms get worse when the stop taking them. These
18. medicines have serious, severe side effects. You should be closely monitored by
your doctor.
Belimumab (also known as Benlysta™) is currently being studied in Phase III clinical trials to
determine whether or not it is effective for lupus. Belimumab specifically reduces the
actions of a protein called “B lymphocyte stimulator,” or BLyS. BLyS is a protein that
increases the lifespan and inflammatory potential of certain immune cells called B cells,
which are known to be hyperactive in lupus patients. Belimumab, which interferes with
BLyS, is a human antibody. This means that it looks a lot like the antibodies that the immune
system makes to fight off viruses. But in this case, belimumab targets only the protein BLyS.
Because it only has one target, it is called a “monoclonal” antibody.
It is important for a person with SLE to have:
Preventive heart care
Up-to-date immunizations
Tests to screen for thinning of the bones (osteoporosis)
Conventional Treatment for Lupus Nephritis differs slightly.
The goal of treatment is to improve kidney function and to delay kidney failure.
Medicines may include corticosteroids or other medications that suppress the immune
system, such as cyclophosphamide,mycophenolate mofetil, or azathioprine.
A person with Lupus may need dialysis to control symptoms of kidney failure, sometimes for
only a while. A kidney transplant may be recommended. People with active Lupus should
not have a transplant because the condition can occur in the transplanted kidney.
Conventional Treatment thatIhave been prescribed has includedcorticosteroids,
Hydroxychloroquine,2different bloodpressure medications, several different painkillers
as well asanti-inflammatory medication and differentdiuretic medication. Thepainkillers
andanti-inflammatory medication was theonlymedication thathashada measure of
success in treating thesymptoms.
19. PROGNOSIS –EXPECTATIONS & OUTCOME
How well a person does depends on the severity of the disease.
The outcome for people with SLE has improved in recent years. Many people with SLE have
mild symptoms.
Quality of life and life expectancy for people with SLE varies greatly, based on the severity of
the illness and how long the disease is present before diagnosis and treatment begins. The
extent to which the disease has progressed at the onset of treatment greatly impacts the
life expectancy for SLE patients. When diagnosed early, Lupus can be treated and brought
largely into remission before the occurrence of serious organ damage. However, left
untreated over a period of time, Lupus can lead to serious problems with vital internal
organs, including the brain, heart, lungs, and kidneys. Such damage can severely
compromise the life expectancy for Lupus patients.
About 50 % of SLE patients will have a neuropsychiatric disorder such as seizures,
memory loss, headaches, or depression.
Women with SLE have an increased risk of developing heart disease.
Between 40 and 60 % of SLE patients have some form of photosensitivity.
About 10% of people with SLE will have symptoms of one or more other connective
tissue diseases.
Lupus deaths have increased 61 % since 1980.
Lupus deaths are 5 times higher in women than in men.
Of all SLE deaths, 36.4% occurred among people aged 15-45 years.
20. Lupus deaths are three times higher in black people than in white people.
21. During 1979-1998, the annual number of deaths increased from 879 to 1,406, and the crude death
rate increased from 39 to 52 per 10 million population, with 22,861 deaths reported during the
study period.
* per 10 million population
COMPLICATIONS
There are several complications associated with SLE, depending on which systemor organ is
being affected.
Some people with SLE have abnormal deposits in the kidney cells. This leads to a condition
called Lupus Nephritis. People with this condition may eventually develop kidney failure and
need dialysis or a kidney transplant when they reach end-stage renal disease.
22. Other complications may include:
Blood clots in the legs (deep vein thrombosis) or lungs (pulmonary embolism)
Destruction of red blood cells (haemolytic anaemia) or anaemia as a chronic
disease
Fluid around the heart pericarditis, endocarditis, or inflammation of the heart,
myocarditis.
Fluid around the lungs (pleural effusions) and damage to lung tissue
Pregnancy complications, including miscarriage
Stroke
Severely low blood platelets (thrombocytopenia)
Inflammation of the blood vessels
ALTERNATIVE APPROACH AND THERAPIES
More and more people with Lupus are turning to natural or alternative remedies to treat
their Lupus as conventional medication has side effects on many people. Diet seems to be a
huge factor in preventing and controlling Lupus flare-ups. It has been proven that
maintaining the body’s PH balance close to 7.5 has very good results in keeping flare-ups at
bay.
If a person chooses to take the dietary and natural route for treatment, their change should
be total or no progress will be made.
A typical diet for Lupus would be made up of vegetable and fruit juices and a good vitamin
and mineral supplement. All meat, gravy, fats, junk food, fried food, soft drinks, caffeine,
and alcohol has to be eliminated from the diet. If kidneys are affected, salt should be
eliminated as well.
A vegetable juice fast is very helpful.
Echinacea, yucca, red clover, and goldenseal are helpful herbs to include into the diet.
70% of the diet should consist of fresh foods.
All fats except for flaxseed, because of its high omega 3 content should be avoided.
23. Food and substances to avoid include:
Alfalfa sprouts as they contain canavain. Canavain can produce Lupus-like symptoms
Nightshade plants and vegetables. These include eggplant, tomatoes, tobacco, sugar
products, white potatoes and any pepper. These contain solanine, which will
increase inflammation and pain.
Birth control drugs
Corticosteroid drugs as they weaken the bones and immune system
Allergenic cosmetics
Ultraviolet rays especially fluorescent lights and strong sunlight
Allergy causing foods and substances such as beef, cow’s milk, wheat, corn,
ammonia, hair spray, formaldehyde, perfume, ethanol and pesticides.
Relative success in controlling symptoms and flare-ups has been achieved with the use of
Ozone Therapy. Ozone is an activated, trivalent (three atoms) form of oxygen. Oxygen is O2
whereas ozone is O3. Over a period of 20-30 minutes, ozone breaks down into two atoms of
regular oxygen - by giving up one atom of singlet oxygen leaving a single, reactive oxygen
atom. Medical ozone is made when medical grade oxygen is electrically activated (using an
ozone generator) to form ozone. Ozone is germicidal, bactericidal, and fungicidal. Oxygen
has these properties too, but less strongly. Ozone therapy has been used in medical and
naturopathic medicine since the 1870's.
Kinesiology sessions are also very helpful in controlling symptoms of Lupus. A good point to
start at is with N.O.T, at least 3 sessions, after which it is advisable to continue with Neuro
Balances in order to get to and defuse the Emotional issues involved with the particular type
of Lupus that the person is suffering from. This has proved very successful in a number of
cases.
Lupus sufferers should also get enough rest and avoid stress at all cost. Getting the proper
amount of rest is extremely important for people with Lupus, especially during periods of
flare-ups. Damaged and inflamed muscles and joints require rest to heal. Rest is also vital in
reducing fatigue. Although everyone has his or her own particular sleep requirements, at
least seven hours of sleep a night is recommended for people with Lupus. It is also
important to be aware that too much sleep isn’t healthy either. Spending all day in bed may
make muscles weaker, which can contribute to feelings of fatigue. Napping during the day
24. may be helpful and even necessary when Lupus activity is causing a flare. A sufferer should
try to allow extra time in their daily schedule for rest.
Exercise is also beneficial to Lupus sufferers, although strenuous exercise should be avoided
if the heart is in any way affected by the disease.
When you’re living with Lupus, the very thought of exercising can be painful. You’re tired,
your joints ache, and you just want to rest. But research shows that exercise can help
people with Lupus build stronger muscles, prevent joint stiffness, control fatigue, and avoid
weight gain and depression. Sufferers should be sure to consult with their doctor first
because some movements can be harmful when you have swollen joints or muscle pain.
If swollen joints or muscle pain are experienced, a person with Lupus should avoid or at
least limit activities that may be demanding on joints and muscles, such as jogging,
weightlifting, or high-impact aerobics.
Recommended exercise should be low impact exercise and can include Yoga, Thai Chi,
Pilates, swimming, stretch exercise and brisk walks. Even everyday activities such as
gardening, walking pets, and doing household chores are associated with lower levels of
distress.
Ihave nowstarted aPH-Alkaline dietwhere all acidic foodshave been removed frommy
diet.I havealso hadtochange thewater thatIdrink andhave tomake surethatI onlydrink
water withaPH above7.This hashad ahugeimpact in improving thearthritis pain Ihave
beensuffering fromfor years.I also takeEchinaforce daily aswell as Flaxseed oil.
Ihave nowworkedin adaily walk withmydogwhich hasimproved myfatigue andmuscle
aches drastically.
Igofor regular Kinesiology sessions andweare working towardsgettingtothebottomof
my emotional issues which iscausing SLEflare-ups. I am also inthe processof investigating
Ozonetherapyandhopetostart thatsoon.
METAPHYSICAL MEANINGS OF LUPUS
25. Depending on which system or organ of the body is affected by Lupus, there are a number
of Metaphysical meanings associated with the disease.
Someone who suffers from Lupus is typically a person who has a self wrongness persona
that can't face things and that can't prioritise or order things. They have very scattered
consciousness trying to do too many things in order to please too many people. Your typical
“People Pleasers”. Usually they have low self esteemand seem to others as if they are
hiding from the world.
People with Lupus also seemto be people who gave up on who they are. They have no
identity.
Rather than fighting for themselves, they seem to be punishing them self. They do not
stand up for themselves in a hostile situation but rather back down and let the other person
feel as if they “won”.
They avoid confrontation with others at all cost. They don’t like fighting and arguing and
believe that nobody will listen to them when they do get involved in an argument.
A person who has Lupus where the skin is affected usually has issues with facing the world
with pride. They are more likely to be embarrassed with who they are. They feel as if they
cannot put up a brave face to face the world. They have a deep need to break out from who
and what they are, but lack the confidence and self esteem.
In some cases they have issues with protection. Protecting themselves from the outside
world is priority and they want to hide away in order to do this.
Usually when the muscles and joints are affected the person with Lupus feels confined. They
have imposed so many restrictions on themselves that they are unable to live life to its
fullest. They are tied down and rigid with their own burdens. They have no balance in their
life and freeze up under stressful situations. Usually they desperately try and stay in control
of their lives, but they always find issues to cramp their style.
Where the Nervous systemis affected, the person suffering from Lupus usually seems to be
out of control and disconnected with life. They have conflict between their thought and
their feelings. “The brain and the heart fighting syndrome”. This makes them feel
overwhelmed to a point where they shut down and close themselves off from the world
around them.
In some cases the eyes are affected and the person has issues looking at the ‘bigger picture’.
They are unfocussed and are unable to think clearly.
Lupus can also affect the lungs, in which case the person suffering from Lupus, has
unresolved issues with grief or guilt, or both. They lack the ability to live life to the full as
26. they feel they have no inspiration. They regret something they have or have not done in
their life and this is stopping them from moving forward.
Sufferers from Lupus Nephritis also seemto carry a lot of shame and self criticism in their
persona. They usually are disappointed in themselves or of something they have or have not
done in their life. They see themselves as failures as at some point in their life they may not
have accomplished a goal they have set for themselves. They do not seem to get over their
personal failures and disappointment, but seemto relive that in all their new undertakings.
They feel like that is the pattern of their life and it cannot be broken.
REFERENCES:
1. Ruiz-Irastorza G, Ramos-Casals M, Brito-Zeron P, Khamashta MA. Clinical efficacy
and side effects of antimalarials in systemic lupus erythematosus: a systematic
review. Ann Rheum Dis. 2010;69:20-28.
2. Hahn BH, Tsao BP. Pathogenesis of systemic lupus erythematosus. In: Firestein GS,
Budd RC, Harris ED Jr., et al., eds.Kelley's Textbook of Rheumatology. 8th ed.
Philadelphia, Pa: Saunders Elsevier; 2008:chap 74.
3. Appel GB. Glomerular disorders and nephrotic syndromes. In: Goldman L, Ausiello
D, eds. Cecil Medicine. 23rd ed. Philadelphia, Pa: Saunders Elsevier; 2007:chap
122.
4. Appel GB, Radhakrishnan J, D’Agti V. Secondary glomerular disease. In: Brenner
BM, ed. Brenner and Rector's the Kidney. 8th ed. Philadelphia, Pa: Saunders
Elsevier; 2007:chap 31.
5. The Natural Remedies Encyclopedia, Seventh Edition by Vance H. Farrell, Harold M
Cherne MD
6. Essentials of Human Anatomy & Physiology, Sixth Edition by Elaine N Marieb
7. Foundations of Anatomy and Physiology, Fifth Edition by Kathleen J. W. Wilson