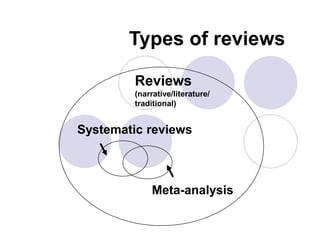
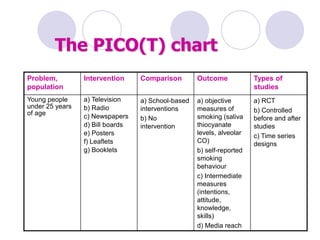
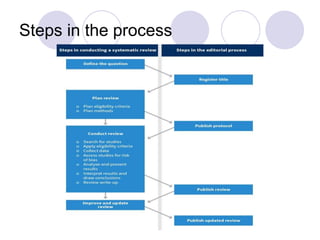
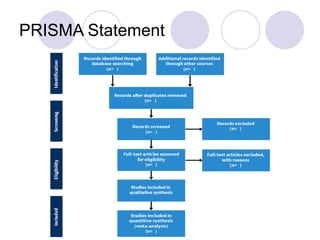
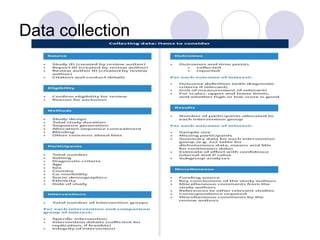
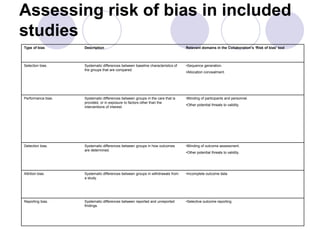
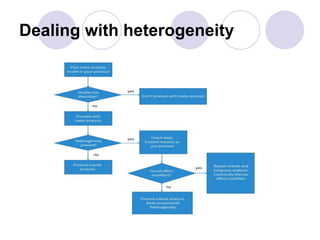
This document provides an overview of systematic reviews and meta-analyses. It defines systematic reviews as reviews that use explicit and reproducible methods to minimize bias in identifying, selecting, and synthesizing studies. Key elements of systematic reviews include formulating a clear question, conducting a comprehensive search, applying objective selection criteria, assessing risk of bias, and synthesizing data, which may include meta-analysis. Heterogeneity and reporting bias are important considerations in analyzing and interpreting systematic review results. The document outlines the process for conducting systematic reviews and meta-analyses.