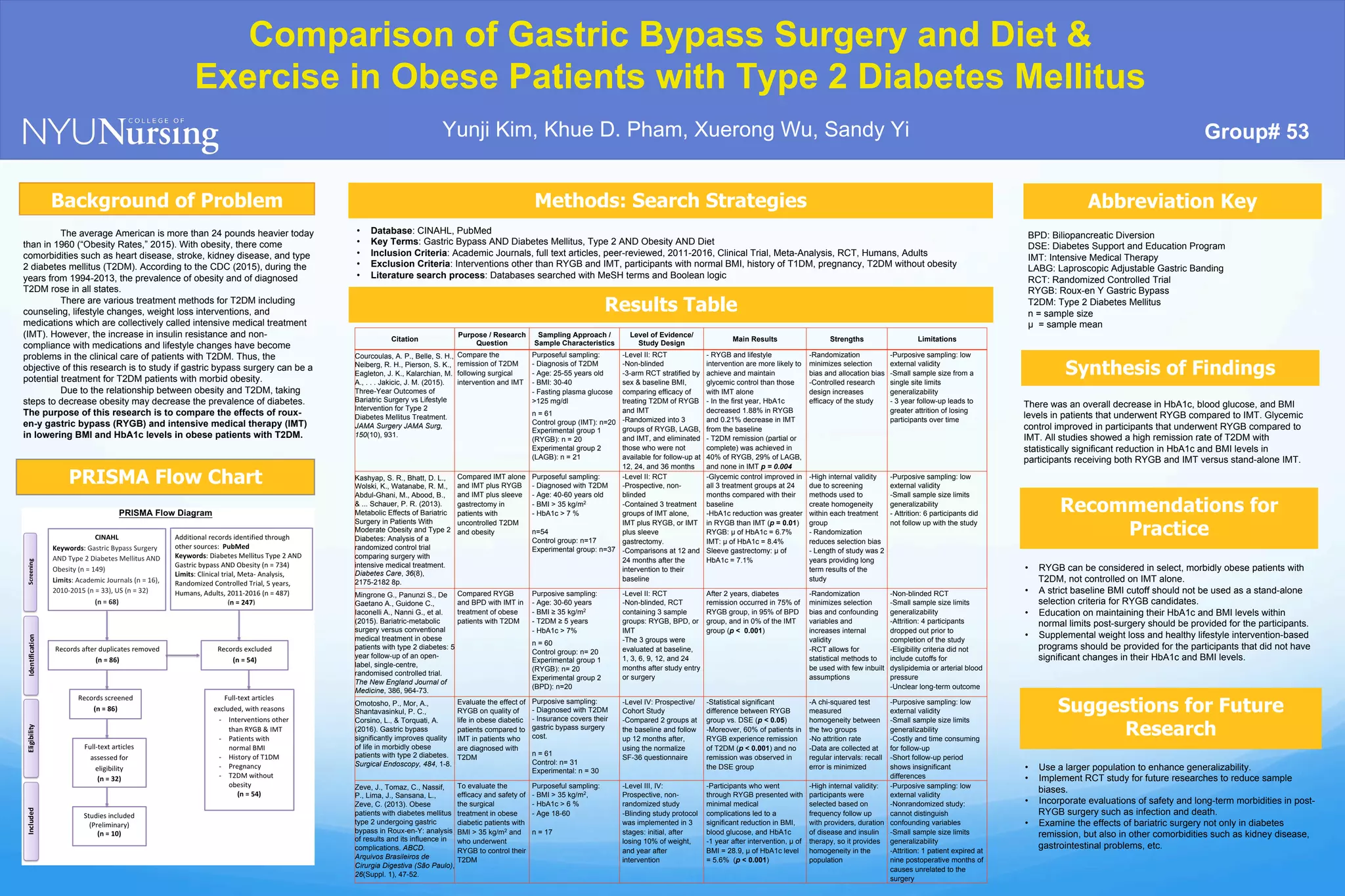
Gastric bypass surgery results in better glycemic control and diabetes remission compared to intensive medical therapy alone in obese patients with type 2 diabetes according to several randomized controlled trials and cohort studies. Studies found greater reductions in HbA1c and BMI levels in patients who underwent gastric bypass surgery versus those receiving intensive medical therapy. Remission rates of type 2 diabetes were higher, ranging from 40-75%, in patients undergoing gastric bypass surgery compared to 0% of those receiving intensive medical therapy alone. However, larger and longer term studies are still needed to further evaluate safety and long term outcomes of gastric bypass surgery.