4. Abdominal examination helps as to identify
abnormalities in the abdomen such as:-
Organ enlargement,
Masses,
Peritoneal irritation,
Hernias,
Fluid accumulation,
Abnormal peristaltic movement.
12/30/2016 4
5. Abdominal examination…Cont’d
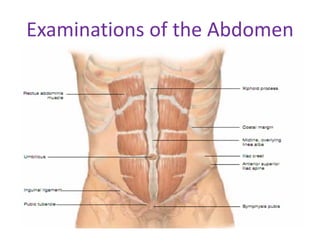
Locating abdominal structures
• Methods of locating abdominal finding is done
by dividing abdomen in to four quadrants by
two perpendicular lines.
• One vertical pass through the umbilicus and
one horizontal line through the umbilicus.
12/30/2016 5
6. RUQ which contain:-
Rt adrenal gland
Liver
Gall bladder
portion of Rt kidney
head of pancreas
Duodenum
Pylorus loop of small intestine
Parts of the colon(hepatic flexure, portion of
transverse and ascending colon ).
12/30/2016 6
7. RLQ-which contain:-
Appendix
distended bladder
Rt ovary
Rt salpinx
Portion of ascending colon
Lower pole of Rt kidney
Cecum
Rt spermatic chord
Rt ureter
Enlarged utrus
Loop of small intestine
12/30/2016 7
8. LUQ- which contains:-
Lt adrenal gland
Portion of Lt kidney
Body of pancreas
Spleen
Stomach
Loop of small intestine
Portion of colon (spleenic flexure, portion of
transverse and descending colon).
12/30/2016 8
9. LLQ-which contain
Distended bladder
Left ovary
Lt salpnix
Lt spermatic chord
Lt ureter
Enlarged utrus
Loop of small intestine
Lower pole of Lt kidney
Sigmoid and portion of descending colon
12/30/2016 9
10. Palpable organs-
Often palpable
Sigmoid colon
Cecum
Iliac arteries
Distended bladder
Pregnant utrus
Pulsation of abdominal
aorta
portion of ascending,
transverse and
descending colon
12/30/2016 10
11. • Rt kidney and liver may palpable only in some pts.
• Much of the liver, much of the stomach and all of
the usual normal spleen are in the abdominal cavity
and extended under the rib cage to the dome of
diaphragm, therefore none palpable.
• Most of the gall bladder lies deep to the liver,
duodenum and pancreas lie deep in the upper
abdomen, hence none of them palpable.
• Techniques of examination
– The usual sequence of inspection, palpation, percussion
and auscultation is modified in the examination of the
abdomen.
– Inspection, auscultation, percussion and palpation.
12/30/2016 11
12. Inspection
• Observe the size and shape of the abdomen:
• it is described as flat, round, or scaphoid.
• Check for symmetry of the abdomen.
• Check for an umbilical hernia.
• A slight pulsation may be noted in the midepigastric
area, particularly in very thin clients. This is the
pulsation of the abdominal aorta.
• In adults, observable veins may reflect major health
problems.
• Increased peristaltic waves of intestinal
obstruction.
• Increased pulsation of an aortic aneurysm.
12/30/2016 12
13. Auscultation
• Auscultation assesses the sounds of peristalsis and vascular
abnormalities.
• Listen for bowel sounds and note their frequency and
character.
• Normal sound consists of clicks and gurgles, the frequency
which has been estimated from 5 to 30 per minute.
• Borborygmus- loud prolonged gurgles of hyper peristalsis.
• Bowel sounds may be altered in diarrhea, intestinal
obstruction, paralytic ileus, and peritonitis.
• Normal blood flow through the abdominal arteries can not be
heard.
• Blood flow through dilated or constricted blood vessels
results in a turbulence that can be detected by auscultation.
12/30/2016 13
14. • Recall that the bell detects low-pitched sounds.
Place the bell of stethoscope over:
– Abdominal aorta in midepigasrium above the umbilicus.
– Renal arteries to the right and left slightly above the
umbilicus.
– Hepatic and splenic arteries in the right and left
hypochondrium.
• To be considered significant, an abdominal bruit
must be heard as the client is moved in to various
positions.
• Friction rub: rough grating sound, occurs with
irritation of the peritoneal surface of an organ,
splenic infarction, primary or metastatic tumor of
liver, and peritonitis.
12/30/2016 14
15. • Percussion
Light percussion of the abdomen is performed to
determine:
– Enlargement of an organ
– The presence of masses
– The presence of abdominal distension or the amount
and distribution of gas in the abdomen.
• A dull percussion note will be heard over the area
of a dense abdominal organ, such as liver or spleen,
and over a solid tumor or fluid.
• Dull percussion notes detected in the suprapubic
area may be from a distended urinary bladder.
12/30/2016 15
16. • Tympany is the normal percussion note present
through out the abdomen except for areas over the
liver, spleen and pubic symphysis.
• With gaseous distension tympany will be elicited
throughout the abdominal area.
• The vertical span of liver dullness represents the
size of the liver in the adult; this is normally about
6-12cm in the mid-clavicular line& 4-8cm in mid
sternal line.
• Vertical span is greater in men than women, tall
person than short.
• Percuss down the right anterior chest in the
midclavicular line (MCL).
12/30/2016 16
17. • Resonance over the lung will be detected until
about the 5th to 7th intercostal space, where liver
dullness begins.
• Continue percussion down ward until the lower
edge of liver dullness is heard. The normal lower
level is at the costal margin.
• Ask the client to inhale, and percuss down ward
again on inspiration, there should be an increase of
about 2 to 4cm from the previous lower edge of
liver dullness, because the liver moves down ward
on inspiration.
12/30/2016 17
18. • In clients with emphysema, the lower level of liver
dullness may be anywhere from 2 to 6cm below the
right costal margin. This is because continued lung
inflation has displaced the liver.
• The span of liver dullness is increased when the
liver is enlarged.
• The span of liver dullness decreased when the liver
is small.
• Dullness of a right pleural effusion or consolidated
lung, if adjacent to liver dullness may falsely
increase the estimated liver size.
• Gas in the colon may produce tymapny in the right
upper quadrant, observe liver dullness and falsely
decrease the estimated liver size.
12/30/2016 18
19. • The spleen lies slightly posterior to the left mid
axillaries line, b/n the 8th and 11th ICS.
• The vertical span of spleen dullness approximately 6 to
8cm in the adult.
• Percussion of spleen does not confirm spleeno-megally
but can raise suspicious.
• For percussion of the spleen, have the client lie slightly
on his right side.
• Percuss posteriorly to the left MAL, about the level of
the nipple (4th ICS), down ward.
• You will hear lung resonance before reaching splenic
dullness. Below the spleen the characteristic tympanic
note of the abdomen will be elicited.
• Below the 12th find dullness is called positive spleenic
percussion sign.
12/30/2016 19
20. Palpation
• The client should be as comfortable and relaxed as
possible.
• Light palpation-feeling the abdomen gently is
especially helpful in identifying abdominal tenderness,
muscular resistance, some superficial organs & masses.
– If resistance is present, try to distinguish voluntary
guarding from involuntary muscular spasm.
– Feel for the relaxation of abdominal muscles that
normally accompanies exhalation.
– Ask the pt to mouth- breath with jaw dropped open,
voluntary guarding usually decreases with this
maneuvers.
– Involuntary rigidity (muscular spasm) typically persists
despite these maneuvers.
– It indicates peritoneal inflammation.
12/30/2016 20
21. • Visceral pain generally is a poorly localized, dull
pain, where as peritoneal pain usually is easily
localized and is described as sharp, stabbing pain.
• Abdominal pain on coughing or with light palpation
suggests peritoneal inflammation.
• Test for rebound tenderness by gently and slowly
pressing the examining hand deep in to the
abdomen away from the site of the pain, quickly
release your hand.
• As the inflamed peritoneum snaps back, the client
with rebound tenderness will experience induced
pain or increased pain, immediately inquire where
the pain is felt.
12/30/2016 21
22. • Deep palpation is usually required to delineate
abdominal masses.
• Again using the palmar surfaces of your fingers, feel
in all four quadrants. Identify any masses and note
their location, size, shape, consistency, tenderness,
pulsations and mobility.
–Note-palpation may not be justified in some
abdominal problems such as appendicitis when
diagnosis is clear and there is risk of rapture with
manipulation.
–clear and there is risk of rapture with
manipulation.
12/30/2016 22
23. Liver
Place your right hand just below the lower right
costal margin with your fingers pointing toward the
client's right shoulder and parallel with the
abdominal rectus muscle.
• Push the fingers deeply in to the abdomen with a
constant pressure and simultaneously push up
under the rib cage.
• Ask the client to take a deep breath: this will cause
the liver to descend.
• On inspiration, the liver below is palpable about
4cm below the right costal margin in the mid
clavicular line.
12/30/2016 23
24. • An obstructed, distended gall-bladder may form an
oval mass below the edge of the liver and merging
with it. It is dull to percussion.
• Tenderness over the liver suggests inflammation, as
in hepatitis, or congestion, as in heart failure.
•Spleen
• The spleen may be palpable in the normal infant
and young child; however, with the older child and
adult, the spleen must be considerably enlarged
before it can be palpated.
• Place your left hand under the client's left flank at
the level of the 11th and 12th ribs.
12/30/2016 24
25. • Push your right hand gently under the left anterior
costal margin.
• Instruct the client to take a deep breath.
• A grossly enlarged spleen will be able to be
visualized as asymmetry, with the entire left side of
the abdomen raised.
• The spleen is a highly vascular organ, if enlargement
is detected, it must be palpated very gently.
• The enlarged spleen below is palpable about 2cm
below the left costal margin on deep breath.
• You should be take a great care to distinguish
enlarged spleen from enlarged left kidney.
12/30/2016 25
26. • The following points help to distinguish the two;
Whether the mass is the spleen or left kidney is
confirmed by radiologist.
Spleen passes the mid lines of the body but the
kidney does not.
Spleen has notch.
• The palpating hand cannot be inserted b/n masses
and lower rib cage in the case of spleen.
There is percussion dullness when spleen is
enlarged.
12/30/2016 26
27. • kidneys
– They may be felt in children and in adults with scaphoid
abdomens.
– Palpation of the right kidney:
• Although kidneys are not usually palpable, you
should learn and practice the techniques.
• Place your left hand behind the pt just below and
parallel to the 12th rib, with your fingertips just
reaching the costovertebral angle.
• Lift, trying to displace the kidney anteriorly.
• Place your right hand gently in the right upper
quadrant, lateral and parallel to the rectus muscle.
12/30/2016 27
28. • Ask the pt to take a deep breath.
• At the peak of inspiration, press your right hand
firmly and deeply in to the right upper quadrant,
just below the costal margin, and try to capture the
kidney between your two hands.
• Causes of kidney enlargement include
hydronephrosis, cysts, and tumors.
• Bilateral enlargement suggests poly cystic disease.
12/30/2016 28
29. Palpation of the left kidney
• To capture the left kidney, move to the pt’s left side.
• Use your right hand to lift from in back, and your
left hand to feel deep in the left upper quadrant.
• Instruct the client to take a deep breath while you
apply pressure with the examining hand.
12/30/2016 29
30. • Assessing kidney tenderness
• Use fist percussion- place the ball of your hand in
the costovrtebral angle and strike it with the ulnar
surface of your fist.
• Pain with pressure or with fist percussion in the
costovertebral angle suggests kidney infection, but
it may also have a musculoskeletal cause.
• Urinary bladder
–The bladder is non palpable unless it is
distended well above the pubic symphysis.
12/30/2016 30
31. • ABDOMINAL EXAMINATION: SPECIAL TECHNIQUES
1. To Assess Possible Ascites
• A protuberant abdomen with bulging flanks
suggests the possibility of ascitic fluid
• The presence and extent of ascites are assessed by
perccusing the abdomen for shifting dullness or by
detecting a fluid wave.
A. Test for shifting dullness.
• After mapping the borders of tympany and dullness, ask
the pt to turn on to one side percuss and mark the borders
again.
• In ascites, dullness shifts to the dependent side, while
tympany shifts to the top.
12/30/2016 31
32. B. Test for a fluid wave
• An assistant’s hand is placed along the pt’s midline
of the abdomen.
• This pressure helps to prevent the fluid wave from
being transmitted through the tissues of the
abdominal wall. The examiner places the hands
along the side of the pt’s flank, then strikes or tap
one flank sharply, feel on the opposite flank for an
impulse transmitted through the fluid.
• A fluid wave is likely to be found only when there is
a large amount of fluid present.
12/30/2016 32
33. 2. To identify an organ or amass in an ascetic
abdomen.
• Try to ballotte the organ or mass, exemplified here
by an enlarged liver.
• Straighten and stiffen the fingers of one hand
together, place them on the abdominal surface, and
make a brief jabbing movement directly toward the
anticipated structure.
• This quick movement often displaces the fluid so
that your finger tips can briefly touch the surface of
the structure through the abdominal wall.
12/30/2016 33
34. 3. To assess possible appendicitis
• Ask the patient to point to where the pain
began and where it is now.
• Ask the patient to cough.
• Determine whether and where pain results.
• The pain of appendicitis classically begins near
the umbilicus and then shifts to the right
lower quadrant, where coughing increases it.
12/30/2016 34
35. –Search for an area of local tenderness
• Localized tenderness anywhere in the right lower
quadrant may in dictate appendicitis.
• Feel for muscular rigidity
• Early voluntary guarding may be replaced by
involuntary muscular rigidity
• Check the tender area for rebound tenderness
• Rebound tenderness suggests peritoneal
inflammation, as from appendicitis.
12/30/2016 35
36. • Check for Rovsing’s sign and for referred rebound
tenderness.
• Press deeply and evenly in the LLQ and quickly
withdraw your finger. Pain in the right lower guardant
during left- sided pressure suggests appendicitis (a
positive Rovsing’s sign). Rt quadrant pain quickly
withdrawal termed as rebound tenderness.
• Look for a psoas sign. Place your hand just above the
pt’s right knee and ask the pt to raise that thigh against
your hand.
• Increased abdominal pain on this maneuver constitutes
a positive psoas sign, suggesting irritation of the psoas
muscle by an inflamed appendix.
• Cutaneouse hyperesthesia
• Obturator sign
12/30/2016 36
37. 4. To assess possible acute cholecystitis
• Cholecystitis may be detected by pressing the
fingers gently in to the right hypochondrium as the
patient takes a deep breath in, a sudden catch of
breath when the gallbladder touches your fingers
indicates inflammation (a positive Murphy’s sing).
5. To assess ventral hernias
– If you suspect this type of hernia but do not see an
umbilical or incisional hernia, ask the patient to raise
both head and shoulders off the examination coach.
– The bulge of a hernia which usually appear with this
action.
12/30/2016 37
38. 6. To distinguish an abdominal mass from a mass in
the abdominal wall.
– Ask the patient either to raise the head and shoulders or
to strain down, thus tightening the abdominal muscles.
Feel for the mass again.
– A mass in the abdominal wall remains palpable an intra
abdominal mass is obscured by muscular contraction.
12/30/2016 38
39. 7. Localized bulges in the abdominal wall
• Include ventral hernias and subcutaneous tumors
such as lipomas.
– The more common ventral hernias are umbilical,
incisional, and epigastric.
– Hernias usually become more evident when the patient
raises head and shoulders from a supine position.
• Lipomas, small or large, they are usually soft and
often lobulated. When your finger presses down
the edge of lipoma the tumor usually slips out from
under it.
12/30/2016 39
40. 8. Sounds in the abdomen
a. Bowel sounds
• May be increased in clients with diarrhea or early
intestinal obstruction.
• Decreased, in paralytic ileus and peritonitis.
• High-pitched tinkling sounds suggest intestinal fluid
and air under tension in a dilated bowel.
b. Bruits
• A hepatic bruit suggests carcinoma of the liver or
alcoholic hepatitis.
• Arterial bruits with both systolic and diastolic
components suggest partial occlusion of the aorta
or large arteries.
12/30/2016 40
41. 9. Tender abdomens
• Abdominal wall Tenderness
• Tenderness may originate in the abdominal wall.
• When the patient raises head and shoulders, this
tenderness persists; whereas tenderness from a
deeper lesion decreases.
a. Visceral tenderness: Example – Enlarged liver may
be tender to deep palpation.
b. Tenderness from disease in the chest and pelvis
12/30/2016 41
42. • Acute pleurisy
– Abdominal pain and tenderness may be due to acute
pleural inflammation.
• Acute salphingitis
• Frequently bilateral, the tenderness of acute
salphingitis is usually maximal just above the
inguinal ligaments.
12/30/2016 42
43. • Tenderness of peritoneal inflammation
• Severe than visceral tenderness.
• Muscular rigidity and rebound tenderness are
frequently present.
10. Liver enlargement
• A palpable liver does not necessarily indicate
hepatomegaly.
• Clinical estimates of liver size should be based on
both percussion and palpation.
12/30/2016 43
44. A. Down wards displacement of the liver by a low
diaphragm.
• Common finding in emphysema.
• The liver edge may be readily palpable well below
the costal margins.
B. Normal variations in liver shape
• In some persons, especially those with a lanky
build, the liver tends to be somewhat elongated so
that its right lobe is easily palpable as it projects
downward toward the iliac crest.
• Riedel’s lobe – represents a variation in shape, not
an increase in liver volume or size
12/30/2016 44
45. C. Smooth large non tender liver
• Cirrhosis may produce an enlarged liver with a
firm non tender edge.
• Many other diseases may produce similar finings.
D. Smooth large tender liver
• An enlarged liver with a smooth tender edge
suggests inflammation, as in hepatitis, venous
congestion, as in right sided heart failure.
12/30/2016 45
46. E. Large irregular liver
• An enlarged liver that is firm or hard and has an
irregular edge or surface suggests malignancy.
• There may be one or more nodules.
• The liver may or may not be tender.
12/30/2016 46
47. The Anus and Rectum:
• The left lateral position is best for routine examination of
the rectum.
• The buttocks should be separated to inspect the perianal
area and anus. Note is made of any abnormalities of
• the perianal skin
• the presence or absence of
perianal skin tags
perianal warts
fistula in anovaginal wall
pilonidial sinus
anal fissure
perianal hematoma
prolapsed strangulated piles
perianal abscesses
48. • Anal musculature tone is assessed, and the finger rotated 3600
in the canal to feel for any thickening or irregularity of the wall.
• The finger is then passed into the rectum and the rectal wall
assessed with sweeping movements of the finger through 3600.
• With this maneuver, assess
• • texture of the wall
• • area of tenderness
• irregularity of rectal mucosa
• presence of any mass, ulcers
• mobility of the rectal mucosa
• If you feel a mass at your fingertip, ask the pt to strain down.
This moves the mass down by 2Cm or so.
• In men, the rectovesical pouch, seminal vesicles and the
prostate should be felt anteriorly.
• In women, the cervix is felt as a firm, rounded mass projecting
back into the anterior wall of the rectum.
• On withdrawing the finger, look for evidence of mucus, pus and
blood on examining finger.