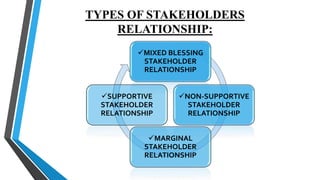
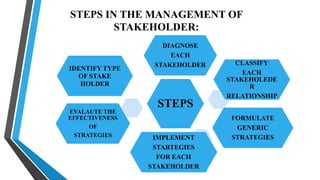
This document discusses major stakeholders in the healthcare system. It defines stakeholders as persons or groups affected by or able to affect organizational actions. There are various types of stakeholders including external (vendors, government), internal (employees, managers), and interface stakeholders. In healthcare, key stakeholders are governmental bodies at central/state/district levels, the public as patients/consumers, healthcare providers like community centers and hospitals, and non-governmental organizations. The document outlines strategies for managing relationships with different stakeholders like collaboration, defense, or monitoring depending on their potential for threat or cooperation.





























































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)






