Download to read offline




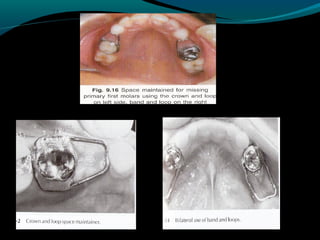
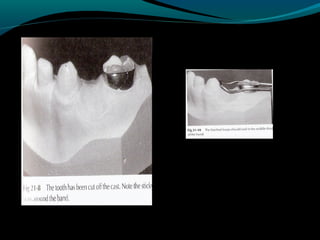


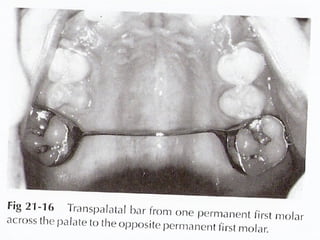
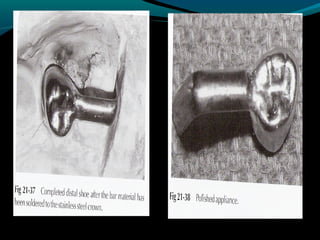
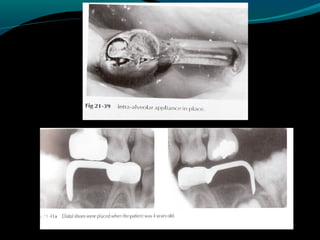



Space maintainers are appliances used to maintain space or regain minor amounts of space lost after a primary tooth is lost. There are several types of space maintainers including fixed appliances like band and loop, lingual arch, and distal shoe appliances as well as removable partial dentures. Key factors in determining the appropriate space maintainer include the time since tooth loss, development of the permanent tooth, and amount of bone covering the unerupted tooth. The document provides details on the construction, advantages, and disadvantages of various space maintainer options.










![Prosthodontic management of endodontically treated teeth [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/prosthodonticmanagementofendodonticallytreatedteethautosaved-210611115147-thumbnail.jpg?width=640&height=640&fit=bounds)






























































