


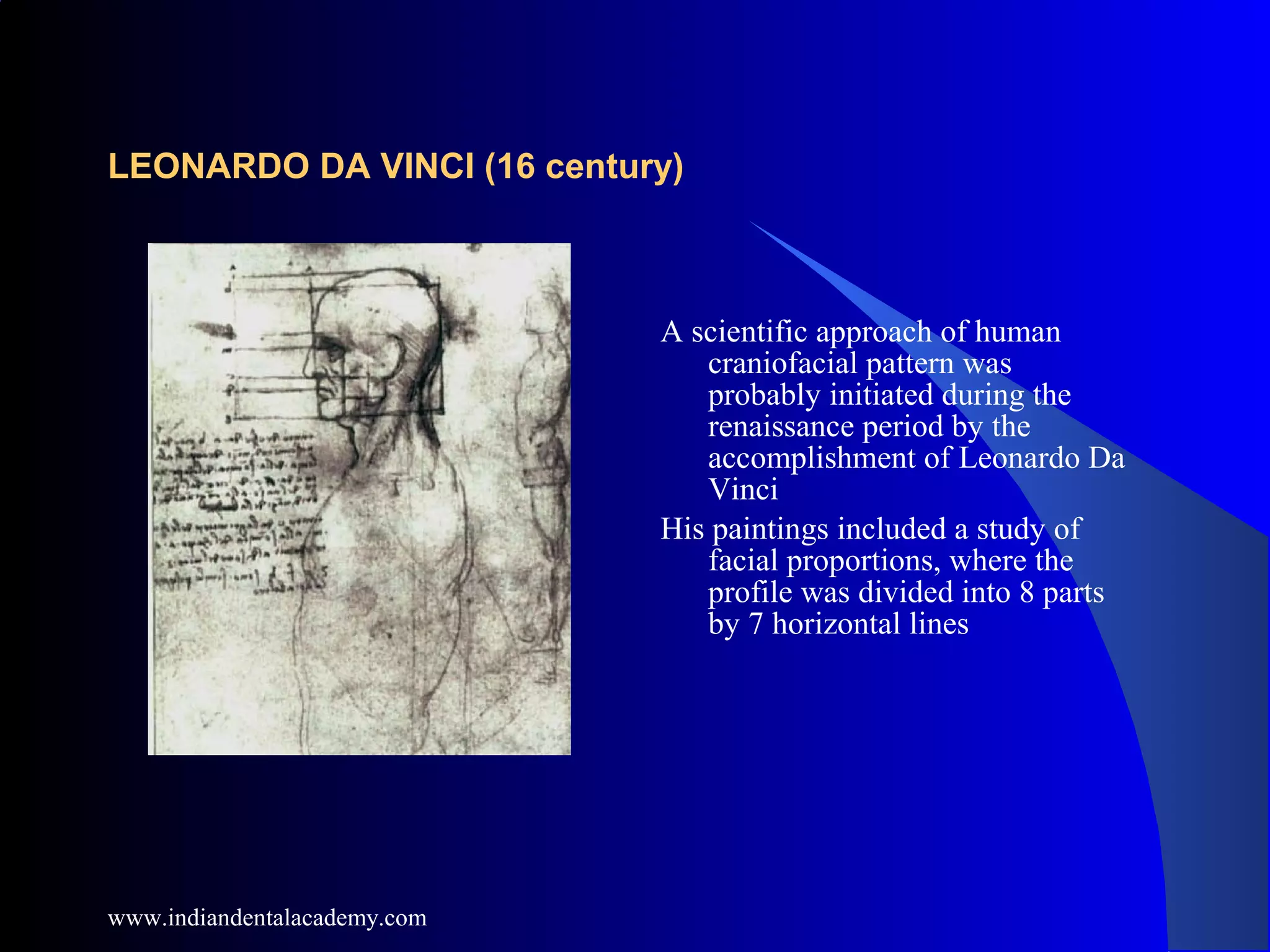































































The document provides a comprehensive overview of soft tissue cephalometric analysis, outlining its historical context, significance, and various analytical methods used in orthodontics. It discusses the inadequacies of traditional osseous analysis and emphasizes the importance of assessing soft tissue for achieving facial esthetics and harmony. Key topics include facial proportions, specific landmarks, and various analyses that inform treatment planning for orthognathic surgery and malocclusion.





































![Soft tissue cephalometric analysis [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/softtissuecephalometricanalysisautosaved-250708101220-a738d47e-thumbnail.jpg?width=640&height=640&fit=bounds)

















































