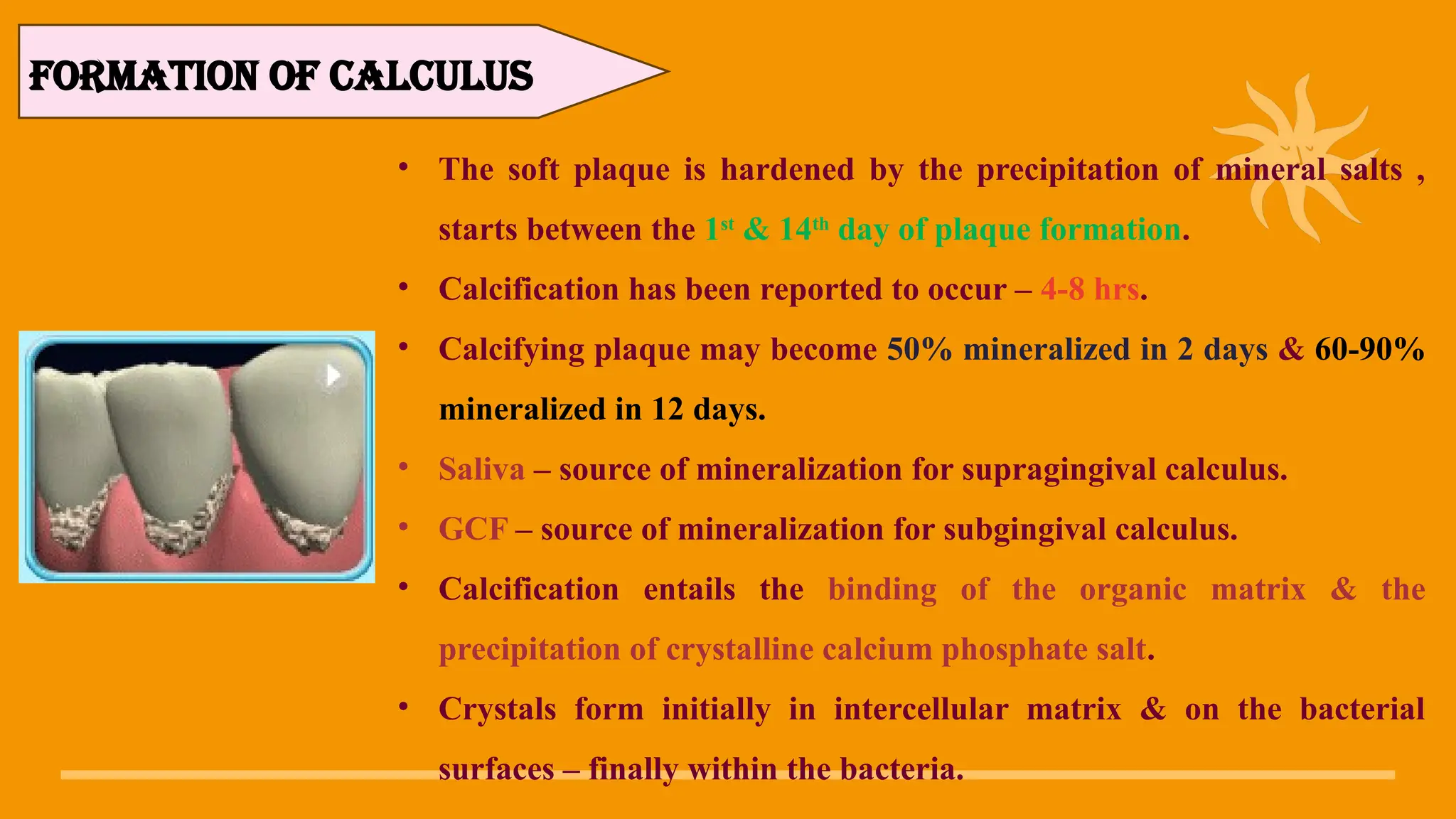
Dental calculus, also known as tartar, is a hardened form of dental plaque that accumulates on the teeth and along the gumline. It forms when plaque, a sticky biofilm composed of bacteria, food particles, and saliva, mineralizes due to the presence of calcium and phosphate in saliva. This process can occur within a few days if plaque is not removed through proper oral hygiene.