Download to read offline

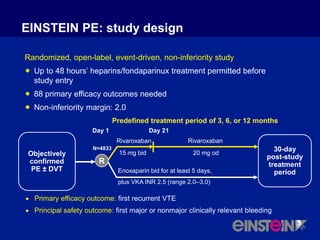
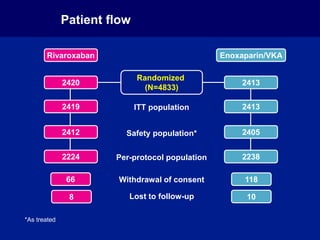
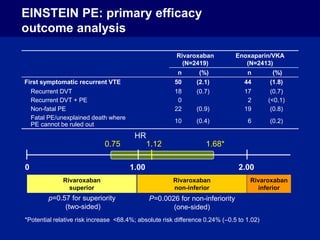
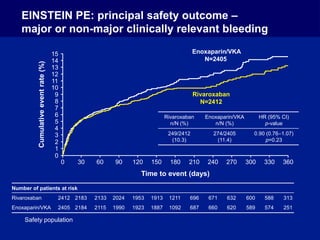
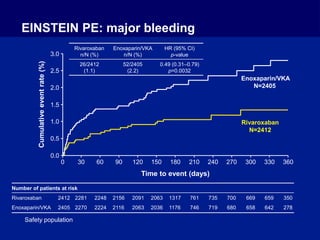

The EINSTEIN PE study evaluated oral rivaroxaban for treating symptomatic pulmonary embolism, demonstrating its non-inferiority to enoxaparin/VKA in efficacy with similar safety outcomes. Rivaroxaban showed significant superiority in reducing major bleeding events compared to enoxaparin/VKA. Overall, rivaroxaban's results were consistent across various patient demographics without indications of liver toxicity.


















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















