This document discusses how accurately capturing HCC (Hierarchical Condition Category) codes is important for health plans to receive appropriate reimbursement from Medicare. It notes that physician coding is often incomplete or inaccurate, resulting in lower payments than plans are entitled to. The document provides examples of common HCCs that are overlooked, such as diabetic manifestations. It emphasizes the need for physician education, coding feedback, and tools to help providers properly document and code HCCs. The document offers specific guidelines and examples regarding coding issues like linkage language, clinical specificity, history of diagnoses, and monitoring conditions treated by specialists. The overall message is that with better training and understanding of HCC coding, health plans can receive full reimbursement for the care their providers
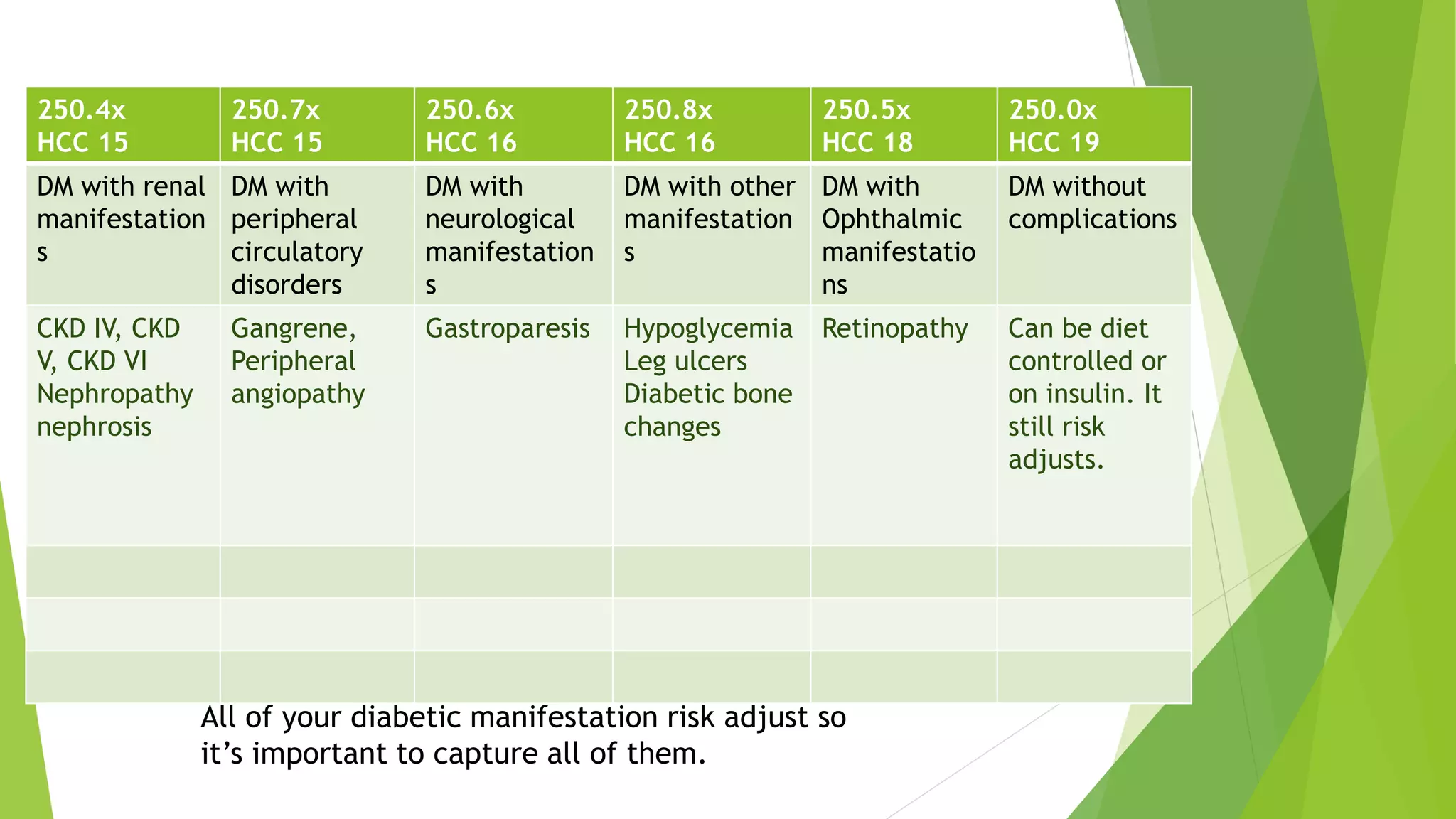
![Educate your providers on how to code their diabetes
codes and also the diabetic manifestations: those
conditions that are “due to” diabetes.
Certified professional coders on staff can perform this
education. Preferably HCC certified coders. Or are you
using Certified coders already to extract the HCC codes?
Give your providers feedback when they forget to
document the diabetic manifestations [and other ICD-9
codes that risk adjust.]
Give your providers positive feedback when they
REMEMBER to document the diabetic manifestations [and
other ICD-9 codes that risk adjust.]
What tools can you use to help your Providers in capturing
their HCC’s?](https://image.slidesharecdn.com/f423922c-7599-43c2-8290-4784acb4f15d-150513005331-lva1-app6891/75/Opal-Conference-Power-Point-1-6-2048.jpg)
![If your diabetic patient has ESRD due to DM and goes on dialysis,
you document this and it is coded as: 250.40, 585.6, V45.11
[renal dialysis status.] 3 codes. Is your Practice doing this?
An HCC that is often documented but not coded is cachexia
799.4. This risk adjusts. You find this most often in your end
stage or cancer patients.
If your patient has hepatitis, cirrhosis or pancreatitis “due to”
alcoholism, you must also code the alcoholism. Even alcoholism
‘in remission’ risk adjusts. Most Providers are not documenting
or coding this. Both drug or alcohol dependence “in remission”
risk adjusts.
A coder can never assume “in remission” vs. “history of” vs.
“current.” Only the Provider knows and can document that. If it
is not documented, you will lose capturing that HCC.](https://image.slidesharecdn.com/f423922c-7599-43c2-8290-4784acb4f15d-150513005331-lva1-app6891/75/Opal-Conference-Power-Point-1-17-2048.jpg)































![Presentation on How to Encounter CMS & HHS RADV Audits [CEU]](https://cdn.slidesharecdn.com/ss_thumbnails/risk-adjustment-webinar-170810065012-thumbnail.jpg?width=640&height=640&fit=bounds)











