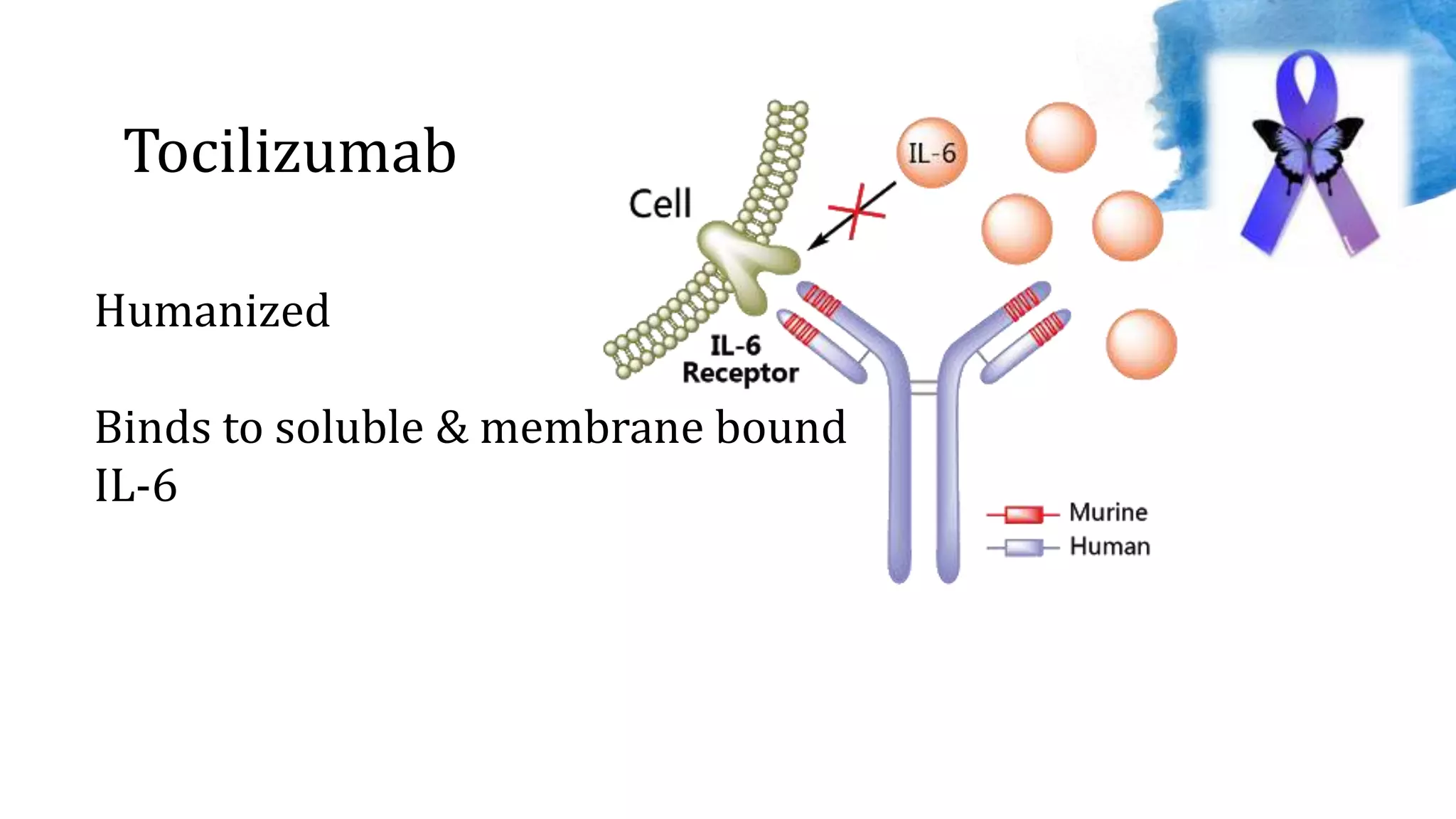
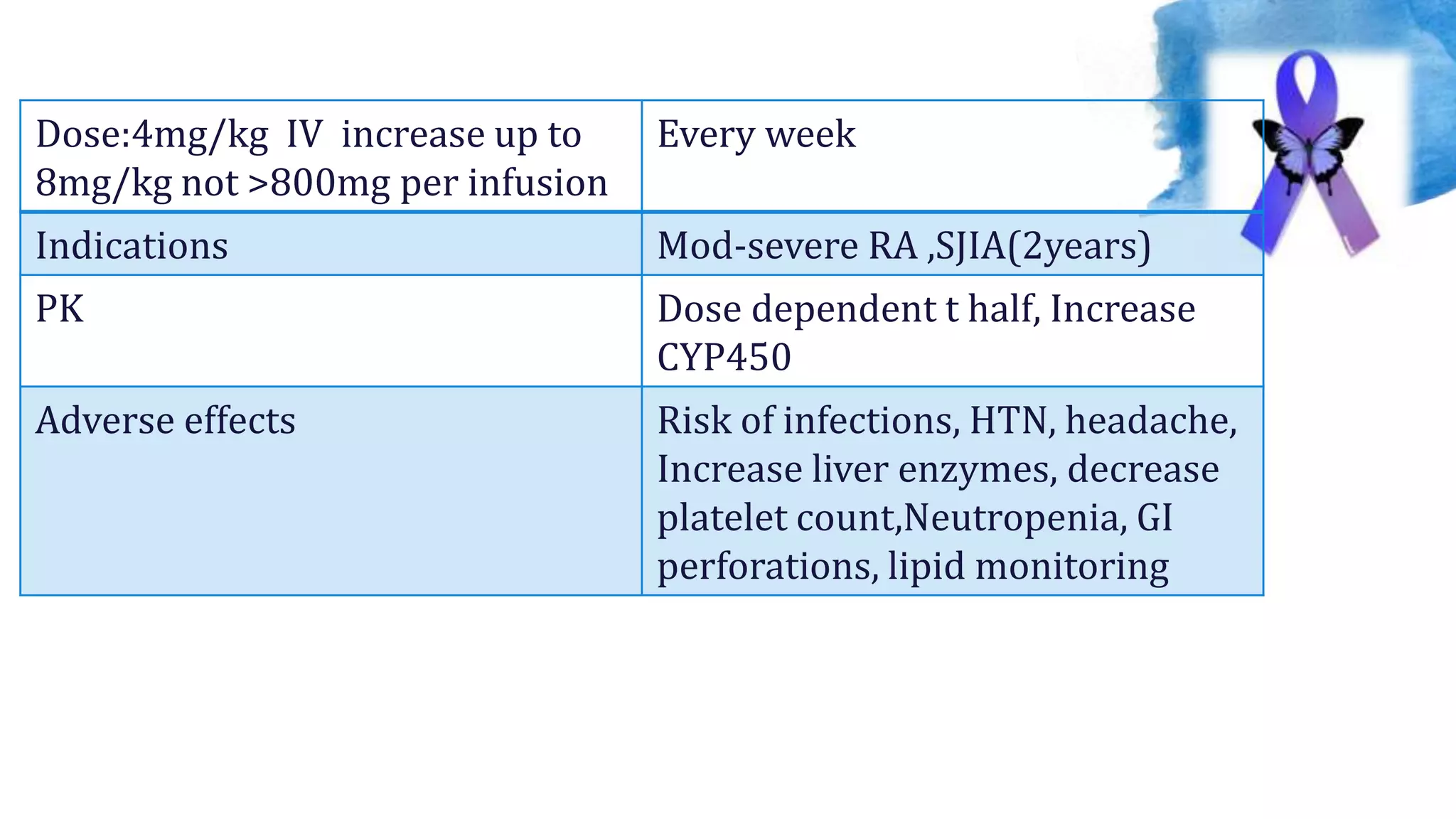
This document discusses biological DMARDs (bDMARDs) for the management of rheumatoid arthritis. It first classifies DMARDs and explains the pathogenesis of RA. It then describes several bDMARDs including their mechanisms of action, dosing regimens, indications, pharmacokinetics, and potential adverse effects. Common bDMARD classes discussed are TNF-alpha inhibitors like adalimumab and infliximab, IL-6 inhibitors like tocilizumab, T-cell and B-cell inhibitors like abatacept and rituximab, and newer targeted bDMARDs. Management guidelines emphasize using methotrexate first followed by bDMARDs if needed.