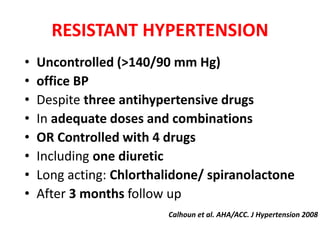
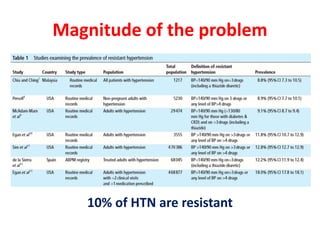
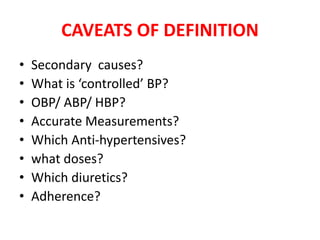
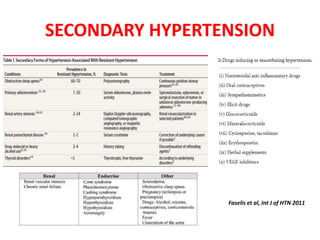
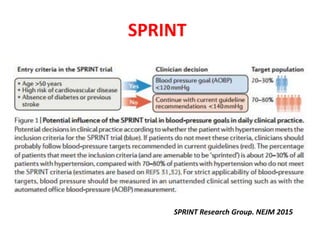
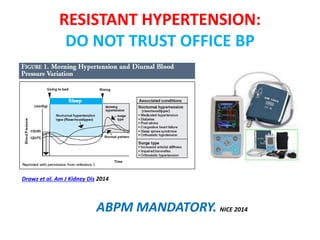
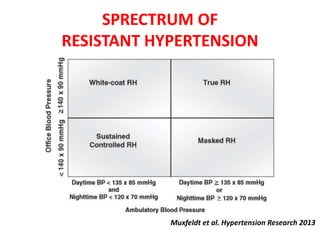
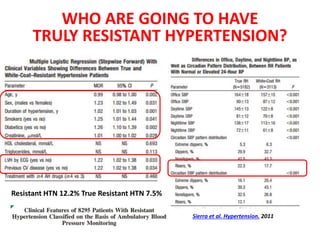
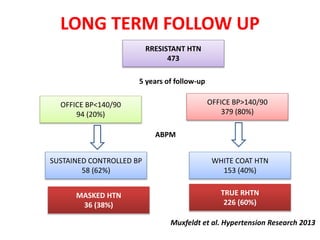
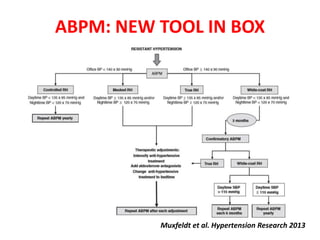
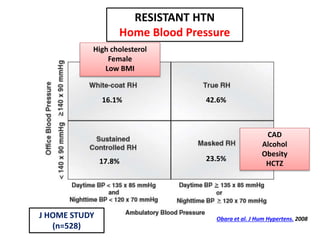
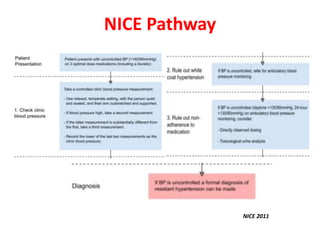
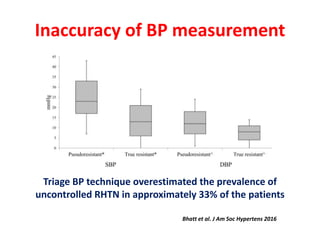
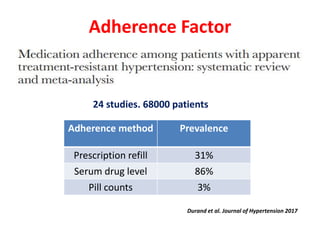
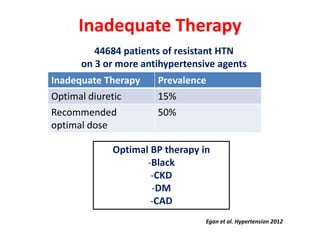
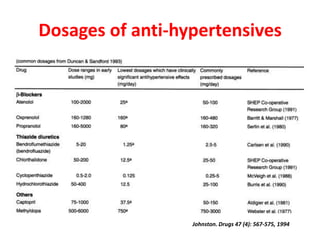
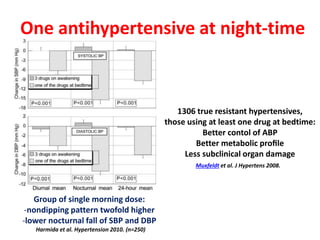
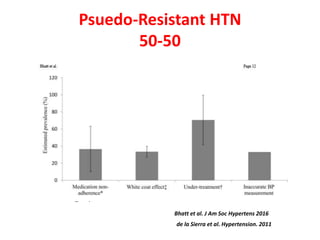
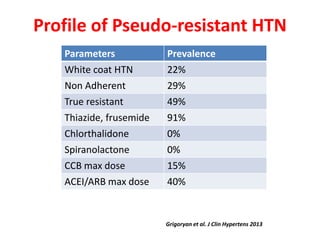
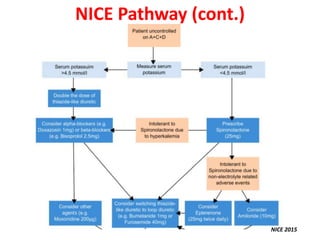
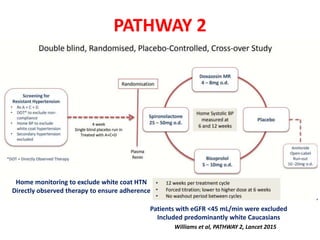
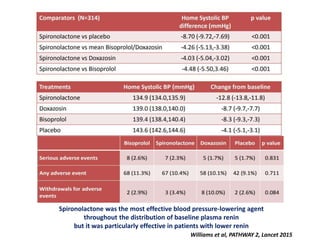
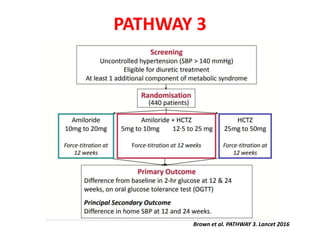
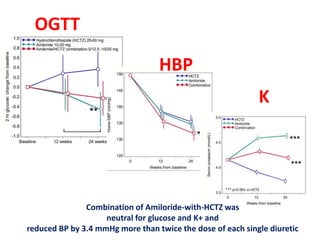
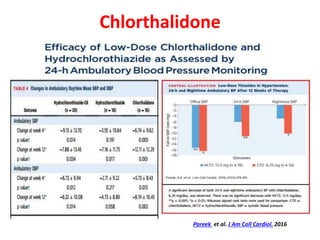
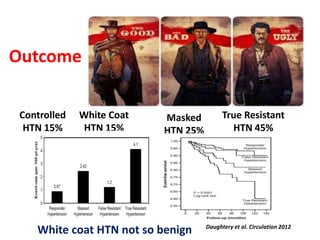
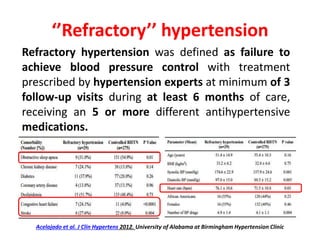
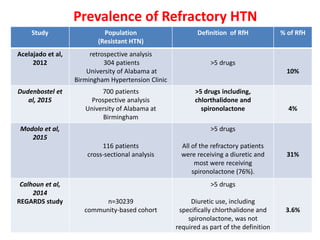
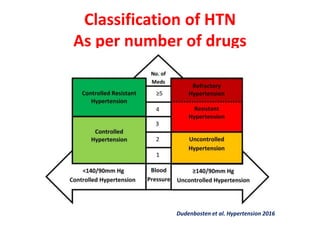
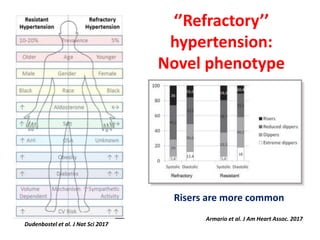
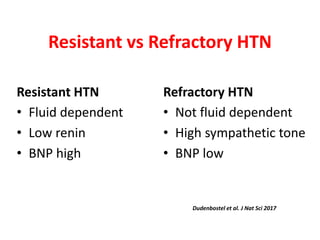
Resistant hypertension is defined as uncontrolled blood pressure despite treatment with three or more antihypertensive medications, including a diuretic. Pseudo-resistant hypertension accounts for around 50% of cases due to issues like inaccurate measurements, poor medication adherence, and inadequate treatment regimens. Ambulatory blood pressure monitoring is important for accurately diagnosing and managing resistant hypertension. Treatment involves optimizing medication regimens with medications like chlorthalidone, spiranolactone, and amiloride-hydrochlorothiazide combinations, and considering interventions for refractory cases involving more than five medications.