Renal function and
testsof renal function
Dr Akeem Oyeyemi Lawal
MBBS (Ilorin), MPH (Manchester), MWACP (LM), FMCPath (Chemical Pathology)
Department of Chemical Pathology
National Hospital Abuja
Lecturer I, Department of Chemical Pathology
College of Health Sciences
University of Abuja
Visiting Consultant Chemical Pathologist
Federal Medical Centre, Jabi
2.
2
Pre-test 1…
Which ofthe following is NOT regarded as a function of the kidney?
A. Fluid balance
B. Synthesis of thrombopoitein
C. Excretion of acid
D. Urine formation
E. Clearance
3.
3
Pre-test 2…
Which ofthe following is most accurate in assessing glomerular
function?
A. Creatinine
B. Cystatin C
C. Para-amino hippuric acid
D. Inulin
E. Iohexol
4.
4
Pre-test 3…
Which ofthe following kidney functions can be inferred from plasma
Calcium assay?
A. Storage function
B. Endocrine function
C. Synthetic function
D. Excretory function
E. Regulatory function
5.
5
Pre-test 4…
‘Electrolyte/urea/creatinine’ isone of the commonly requested
biochemical investigations. What category of kidney function tests can
it be classified?
A. Homeostatic function
B. Synthetic function
C. Excretory function
D. Homeostatic and synthetic function
E. Homeostatic and excretory function
6.
6
Learning objectives
• Toappreciate the functional anatomy of the kidneys
• To understand the physiological roles of the kidneys
• To understand the categories of tests of renal function including
tests of glomerular and tubular function
• To appreciate the application of renal function tests in clinical
practice
9
Introduction
• Renal system:kidneys, ureters, urinary bladder and urethra; accompanying
neurovasculature
• Latter play essentially storage or conduit roles hence renal function is largely
synonymous with kidney function
• Kidneys play a wide array of critical functions including excretory, homeostatic,
synthetic and endocrine functions
• Defects in renal function therefore life-threatening
• Kidney function tests rank most requested biochemical investigations in clinical practice
11
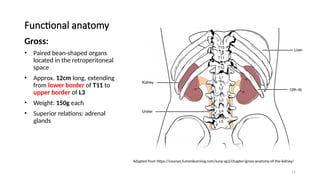
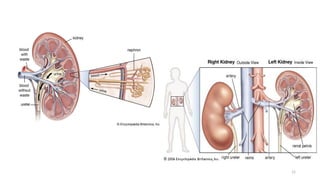
Functional anatomy
Gross:
• Pairedbean-shaped organs
located in the retroperitoneal
space
• Approx. 12cm long, extending
from lower border of T11 to
upper border of L3
• Weight: 150g each
• Superior relations: adrenal
glands
Adapted from https://courses.lumenlearning.com/suny-ap2/chapter/gross-anatomy-of-the-kidney/
12.
12
The Anatomy ofthe Kidney | Interactive Biology, with Leslie Sa
muel (interactive-biology.com)
13.
13
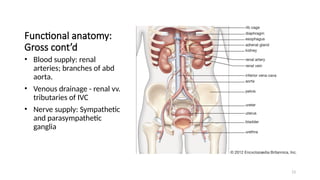
Functional anatomy:
Gross cont’d
•Blood supply: renal
arteries; branches of abd
aorta.
• Venous drainage - renal vv.
tributaries of IVC
• Nerve supply: Sympathetic
and parasympathetic
ganglia
14.
14
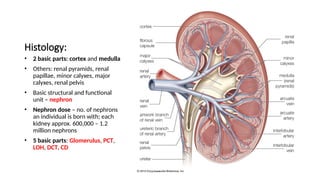
Histology:
• 2 basicparts: cortex and medulla
• Others: renal pyramids, renal
papillae, minor calyxes, major
calyxes, renal pelvis
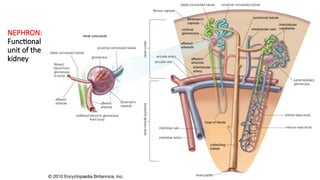
• Basic structural and functional
unit – nephron
• Nephron dose – no. of nephrons
an individual is born with; each
kidney approx. 600,000 – 1.2
million nephrons
• 5 basic parts: Glomerulus, PCT,
LOH, DCT, CD
17
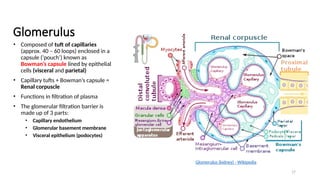
Glomerulus
• Composed oftuft of capillaries
(approx. 40 – 60 loops) enclosed in a
capsule (‘pouch’) known as
Bowman’s capsule lined by epithelial
cells (visceral and parietal)
• Capillary tufts + Bowman’s capsule =
Renal corpuscle
• Functions in filtration of plasma
• The glomerular filtration barrier is
made up of 3 parts:
• Capillary endothelium
• Glomerular basement membrane
• Visceral epithelium (podocytes)
Glomerulus (kidney) - Wikipedia
18.
18
Glomerulus cont’d
• Capillaryendothelium, unlike
others possesses pores (fenestrae)
abt 60nm diameter (size barrier)
• Covered by a ‘gel-like’ substance
(glycocalyx) which possesses
negatively charged
glycosaminoglycans providing
(charge barrier)
• GBM is made up of dense network
of collagen fibres
• Visceral epithelial cells are
referred to as ‘podocytes’ which
have primary and secondary foot
processes that form filtration slits
• Entire structure also covered by
gel matrix and provides a barrier
that is impermeable to substances
≥ 60kDa (Albumin) approx.
diameter 3.5nm
19.
19
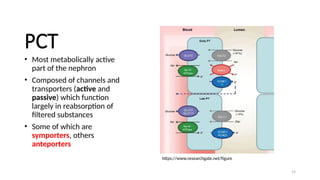
PCT
• Most metabolicallyactive
part of the nephron
• Composed of channels and
transporters (active and
passive) which function
largely in reabsorption of
filtered substances
• Some of which are
symporters, others
anteporters
https://www.researchgate.net/figure
20.
20
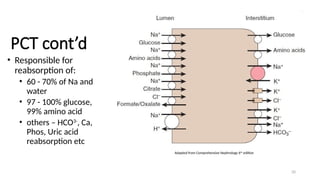
PCT cont’d
• Responsiblefor
reabsorption of:
• 60 - 70% of Na and
water
• 97 - 100% glucose,
99% amino acid
• others – HCO3-
, Ca,
Phos, Uric acid
reabsorption etc
Adapted from Comprehensive Nephrology 6th
edition
21.
21
Loop of Henle…
•‘Hair-pin’ structure
• 2 limbs: Thin descending and thick ascending
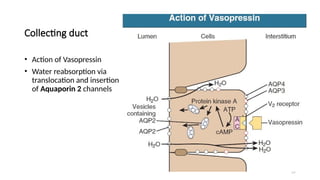
• Thin descending limb is permeable to water, possessing Aquaporin 1
channels
• Thick ascending limb is impermeable to both water and solutes but
possesses transport channels for active efflux of electrolytes (Na, K, Cl)
from the tubular lumen into the peritubular space and ultimately into
peritubular capillaries
• Functions in urine formation by Countercurrent multiplier and
exchanger mechanisms
22.
22
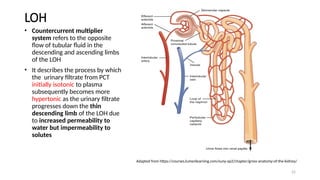
LOH
• Countercurrent multiplier
systemrefers to the opposite
flow of tubular fluid in the
descending and ascending limbs
of the LOH
• It describes the process by which
the urinary filtrate from PCT
initially isotonic to plasma
subsequently becomes more
hypertonic as the urinary filtrate
progresses down the thin
descending limb of the LOH due
to increased permeability to
water but impermeability to
solutes
Adapted from https://courses.lumenlearning.com/suny-ap2/chapter/gross-anatomy-of-the-kidney/
23.
23
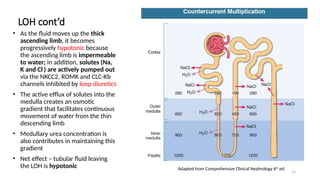
LOH cont’d
• Asthe fluid moves up the thick
ascending limb, it becomes
progressively hypotonic because
the ascending limb is impermeable
to water; in addition, solutes (Na,
K and Cl-
) are actively pumped out
via the NKCC2, ROMK and CLC-Kb
channels inhibited by loop diuretics
• The active efflux of solutes into the
medulla creates an osmotic
gradient that facilitates continuous
movement of water from the thin
descending limb
• Medullary urea concentration is
also contributes in maintaining this
gradient
• Net effect – tubular fluid leaving
the LOH is hypotonic Adapted from Comprehensive Clinical Nephrology 6th
ed.
24.
24
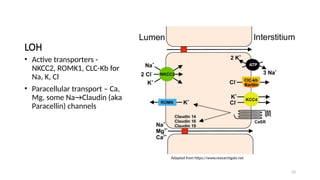
LOH
• Active transporters-
NKCC2, ROMK1, CLC-Kb for
Na, K, Cl
• Paracellular transport – Ca,
Mg, some Na→Claudin (aka
Paracellin) channels
Adapted from https://www.researchgate.net
25.
25
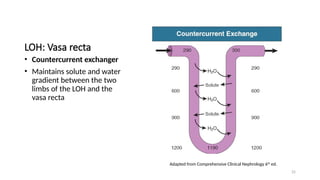
LOH: Vasa recta
•Countercurrent exchanger
• Maintains solute and water
gradient between the two
limbs of the LOH and the
vasa recta
Adapted from Comprehensive Clinical Nephrology 6th
ed.
26.
26
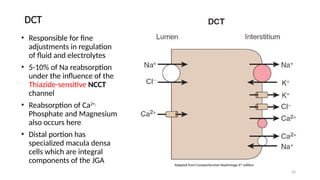
DCT
• Responsible forfine
adjustments in regulation
of fluid and electrolytes
• 5-10% of Na reabsorption
under the influence of the
Thiazide-sensitive NCCT
channel
• Reabsorption of Ca2+,
Phosphate and Magnesium
also occurs here
• Distal portion has
specialized macula densa
cells which are integral
components of the JGA Adapted from Comprehensive Nephrology 6th
edition
27.
27
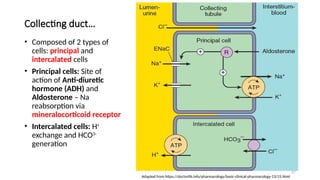
Collecting duct…
• Composedof 2 types of
cells: principal and
intercalated cells
• Principal cells: Site of
action of Anti-diuretic
hormone (ADH) and
Aldosterone – Na
reabsorption via
mineralocorticoid receptor
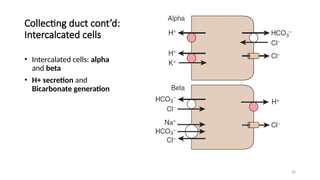
• Intercalated cells: H+
exchange and HCO3-
generation
Adapted from https://doctorlib.info/pharmacology/basic-clinical-pharmacology-13/15.html
31
Functions of thekidney…
1. Homeostatic function: Fluid and electrolyte
balance; Acid-base balance
2. Urine formation
3. Excretory function
4. Endocrine function
5. Synthetic function
32.
32
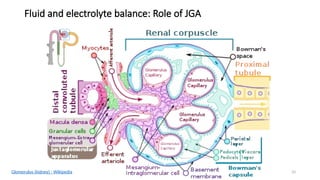
Homeostatic function…
A. Fluidand electrolyte balance:
• Accomplished via the renin-angiotensin-aldosterone system
• Involves the JGA composed of:
• Juxtaglomerular (granular) cells
• Macula densa
• Extra-glomerular mesangial cells of Lacis
• Baroreceptors in the JGA, carotid sinus and aortic arch,
chemoreceptors in the macula densa and osmoreceptors in the
hypothalamus
34
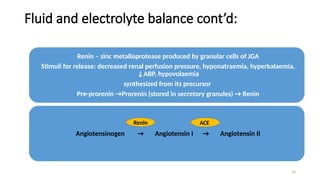
Fluid and electrolytebalance cont’d:
Renin – zinc metalloprotease produced by granular cells of JGA
Stimuli for release: decreased renal perfusion pressure, hyponatraemia, hyperkalaemia,
↓ABP, hypovolaemia
synthesized from its precursor
Pre-prorenin →Prorenin (stored in secretory granules) → Renin
Angiotensinogen → Angiotensin I → Angiotensin II
Renin ACE
35.
35
Fluid and electrolytebalance cont’d:
• Angiotensin II:
• Potent vasoconstrictor
• Stimulates thirst centre
• Stimulates ADH release
• Activates enzyme Aldosterone synthase in the adrenal cortex to synthesize
aldosterone
• ADH – produced in the Supra-optic and paraventricular nuclei (more
in the supraoptic nucleus); stimulus for release in ↑plasma
osmolality >290mOsm/kg
• Aldosterone – produced in the zona glomerulosa of the adrenal
cortex; stimulates Na reabsorption by activating ENaC channel at CD
36.
36
Homeostatic function…
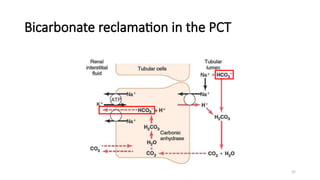
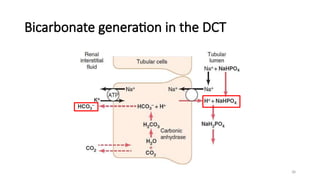
B. Acid-basebalance:
• The kidneys play vital roles in acid-base balance via the ability to
secrete H+
into the urinary filtrate and reclaim, as well as generate
bicarbonate (HCO3
-
) in the PCT and DCT respectively
• It’s large concentration of carbonic anhydrase facilitates these
processes making it the major organ in long-term acid-base control
• The presence of important urinary buffers i.e. ammonium/ammonia
buffer system (NH4
+
/NH3) and phosphate buffer system
(H2PO4
-
/HPO4
2-
) also contribute to its role in acid-base balance
39
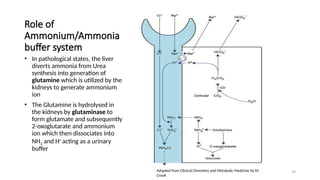
Role of
Ammonium/Ammonia
buffer system
•In pathological states, the liver
diverts ammonia from Urea
synthesis into generation of
glutamine which is utilized by the
kidneys to generate ammonium
ion
• The Glutamine is hydrolysed in
the kidneys by glutaminase to
form glutamate and subsequently
2-oxoglutarate and ammonium
ion which then dissociates into
NH3 and H+
acting as a urinary
buffer
Adapted from Clinical Chemistry and Metabolic Medicine by M.
Crook
40.
40
Urine formation
• Thekidneys are involved in urine formation via the Countercurrent
multiplier and exchanger systems
• Also requires the influence of ADH and Aldosterone
41.
41
Excretory function
• Excretionof metabolic wastes and nitrogenous compounds e.g. Urea,
Creatinine, uric acid, water soluble drugs etc
42.
42
Endocrine function
• Renin
•1,25-(OH)2vitamin D - 1α hydroxylase enzyme
• Erythropoietin
• Thrombopoietin
• Prostaglandins
44
Tests of kidneyfunction…
OUTLINE
• Introduction
• Functional anatomy
• Physiology
• Tests of kidney function
• Clinical applications of renal
function tests
• Conclusion
45.
45
Assessment of glomerularfunction
• Glomerular filtration rate (GFR)
• Concept of clearance
• Markers for clearance studies
• Estimated GFR (eGFR)
46.
46
Glomerular filtration rate
•The kidneys receive 25% of cardiac output
• About 125mL of blood is filtered across the glomerulus per minute
(125mL/min ≡ 180L/day)
• Filtration is dependent on a balance of forces
• Also affected by:
• Renal blood flow
• Renal perfusion pressure
47.
47
Glomerular filtration ratecont’d
• GFR is considered the most reliable measure of functional capacity of
the kidneys
• Reflection of number of functioning nephrons and most sensitive and
specific marker of overall changes in renal function
• Implicated in major classification systems of Acute kidney injury (AKI)
and Chronic kidney disease (CKD) ie. RIFLE/AKIN criteria and CKD-
EPI/KDIGO classification respectively
48.
48
Concept of clearance
•Definition: volume of plasma from which a substance is completely
cleared (removed) per unit time
• Is an index for measurement of GFR
• Requirements for an ideal marker for clearance:
• Stable concentration in plasma – no extra-renal elimination
• Physiologically inert – negligible plasma protein binding
• Freely filtered
• Not reabsorbed
• Not secreted
• Not synthesized
• Not metabolized
49.
49
Formula for clearance
•If criteria fulfilled, for clearance of a substance ‘S’
• GFR x Ps = Us x V (i.e. amount of substance ‘S’ in plasma = amount in
urine)
• Therefore, GFR =
• Where:
• Us – Urine concentration of substance “S”
• Ps – Plasma concentration of substance “S”
• Vt – timed urine volume
50.
50
Classification of markers…
A.Based on source:
• Exogenous
• Non-radioisotopic e.g. Inulin, Iohexol
• Radioisotopic e.g. I-iothalamate, Cr-EDTA, Tc-DTPA
• Endogenous e.g. Creatinine, cystatin C, Urea
B. Based on accuracy of GFR measurement:
• Gold standard – continuous Inulin infusion
• Silver standard – bolus inulin infusion
• Bronze standard – Plasma Creatinine, cystatin C, etc
51.
51
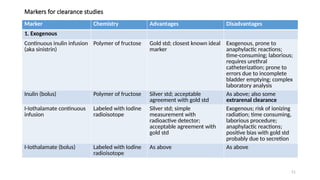
Markers for clearancestudies
Marker Chemistry Advantages Disadvantages
1. Exogenous
Continuous inulin infusion
(aka sinistrin)
Polymer of fructose Gold std; closest known ideal
marker
Exogenous, prone to
anaphylactic reactions;
time-consuming; laborious;
requires urethral
catheterization; prone to
errors due to incomplete
bladder emptying; complex
laboratory analysis
Inulin (bolus) Polymer of fructose Silver std; acceptable
agreement with gold std
As above; also some
extrarenal clearance
I-Iothalamate continuous
infusion
Labeled with Iodine
radioisotope
Silver std; simple
measurement with
radioactive detector;
acceptable agreement with
gold std
Exogenous; risk of ionizing
radiation; time consuming,
laborious procedure;
anaphylactic reactions;
positive bias with gold std
probably due to secretion
I-Iothalamate (bolus) Labeled with Iodine
radioisotope
As above As above
52.
52
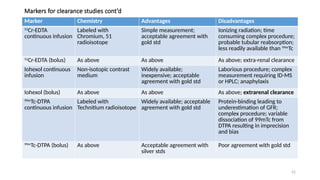
Markers for clearancestudies cont’d
Marker Chemistry Advantages Disadvantages
51
Cr-EDTA
continuous infusion
Labeled with
Chromium, 51
radioisotope
Simple measurement;
acceptable agreement with
gold std
Ionizing radiation; time
consuming complex procedure;
probable tubular reabsorption;
less readily available than 99m
Tc
51
Cr-EDTA (bolus) As above As above As above; extra-renal clearance
Iohexol continuous
infusion
Non-isotopic contrast
medium
Widely available;
inexpensive; acceptable
agreement with gold std
Laborious procedure; complex
measurement requiring ID-MS
or HPLC; anaphylaxis
Iohexol (bolus) As above As above As above; extrarenal clearance
99m
Tc-DTPA
continuous infusion
Labeled with
Technitium radioisotope
Widely available; acceptable
agreement with gold std
Protein-binding leading to
underestimation of GFR;
complex procedure; variable
dissociation of 99mTc from
DTPA resulting in imprecision
and bias
99m
Tc-DTPA (bolus) As above Acceptable agreement with
silver stds
Poor agreement with gold std
53.
53
Markers for clearancestudies cont’d
Marker Chemistry Advantages Disadvantages
Cystatin C Bronze std; endogenous
proteinase inhibitor
Not secreted or reabsorbed; less
influenced by physiological
variation than creatinine;
unaffected by recent meat intake;
internationally standardized assays;
applied in GFR estimating
equations
More expensive than creatinine;
influenced by obesity and thyroid
function; possible influences by
genetic factors
Creatinine
(serum/plasma)
Bronze std; endogenous
nitrogenous substance
synthesize from muscle
protein
Inexpensive; internationally
standardized assays; applied in GFR
estimating equations
Physiological/racial/pathological
variations in GFR-Creatinine
relationship; affected by diet and
meat intake; variable tubular
secretion; variable intestinal losses;
analytical interferences
Creatinine
clearance
As above Inexpensive As above; also requires a timed
urine collection; challenges with
adequacy of urine volume;
cumbersome
Urea Nitrogenous waste product
from ammonia synthesized
in the liver
Endogenous; inexpensive Affected by hydration status, diet;
tubular reabsorption; poor
sensitivity and specificity
Others of uncertain clinical use: β-trace protein, retinol-binding protein, α1-macroglobulin, β2-macroglobulin, Symmetric
dimethyl arginine (SDMA)
54.
54
Creatinine
• Anhydride productof muscle protein creatine
• MW 113Da
• Endogenously produced at a fairly constant rate (1 – 2%
per day)
• Freely filtered at the glomerulus, not reabsorbed
• Cheap, convenient, easy to measure
• Incorporated into many eGFR formulae
55.
55
Creatinine
• However affectedby age, gender, race, muscle mass, nutritional
status, other preanalytical and analytical factors
• Secreted by renal tubules
• Some extrarenal clearance in GIT
• Wide intraindividual variation
56.
56
Cystatin C
• LowMW (12.8kDa) protein synthesized by all nucleated cells
• Functions as a cysteine protease inhibitor
• Endogenously produced at a fairly constant rate
• Freely filtered at the glomerulus, completely reabsorbed and
catabolized by renal tubules hence can also be used as a marker of
tubular function
• Not affected by muscle mass
• However affected by age, gender, weight, height, obesity, thyroid
hormone concentration
57.
57
Urea
• Nitrogenous wasteproduct of protein catabolism
• Synthesized exclusively in the liver
• CO(NH2)2
• Freely filtered at the glomerulus
• Significant tubular “back-diffusion” (passive reabsorption) about 40 –
70% from the tubules into renal interstitium and ultimately into
plasma
• Back-diffusion is reduced in high-flow states e.g. pregnancy due to
increased GFR; reduced in low flow states e.g pre-renal AKI
58.
58
Urea
• Back-diffusion limitsits use as a marker of GFR→ underestimation
• Also significantly affected by protein diet, hydration status, increased
protein catabolism, GI haemorrhage which leads to reabsorption of
blood proteins and treatment with cortisol (or its synthetic
analogues)
• Overall has poor sensitivity and specificity as a marker for GFR and
thus no longer used
59.
59
Urea
• May howeverfind utility in the urea-creatinine ratio to crudely
differentiate pre-renal from intrinsic AKI
• Normal urea-creatinine ratio in a normal individual with normal
dietary intake = 49 – 81 mmol Urea/mmol Creatinine (12 – 20
mg/mg)
• Ratio >81 mmol/mmol said to be suggestive of pre-renal AKI
• Also useful in assessing adequacy of dialysis using the urea reduction
rate ((pre dialysis urea – post dialysis urea)/pre dialysis urea x 100%)
60.
60
Tests of tubularfunction
• Involves evaluation of proximal tubular function (i.e. tubular handling
of sodium, glucose, phosphate, calcium, bicarbonate and amino acids)
and distal tubular function (urinary acidification and concentration)
• Increased levels in urine indicate tubular dysfunction
• Examples:
• Urinary β2-macroglobulin
• Urinary N-acetyl-β-D-glucosaminidase
• Urinary Cystatin C
61.
61
Estimated glomerular filtrationrate (eGFR)
• Developed due to limitations of collection of timed urine specimen for
clearance studies
• Estimate of GFR using mathematical formulae derived from
comparison with clearance studies
62.
62
Estimated glomerular filtrationrate (eGFR)
• Cockcroft-Gault equation
• Modification of diet in renal disease (MDRD)
• CKD-EPI Creatinine (2009)
• CKD-EPI Cystatin C (2012)
• CKD-EPI Creatinine-Cystatin C (2012)
• CKD-EPI Creatinine (2021)
• Schwartz formula (children)
63.
63
Cockcroft-Gault equation
• Oldestequation
• Estimates GFR using weight, age, serum creatinine
• Cohort used did not include women
• Requirement of weight made utility cumbersome
• Was derived using creatinine clearance rather than a reference
method for creatinine
• Did not account for body surface area (BSA)
64.
64
Cockcroft-Gault equation
• Formula:males…
[(140 - age) x weight x 1.23]/serum creatinine (in µmol/L)
OR [(140 - age) x weight/72 x serum creatinine (in mg/dL)]
• Multiply by a factor of 0.85 in females
65.
65
MDRD
• Modification ofdiet in renal disease
• Does not require weight
• Also adjusts eGFR with BSA
• Original formula used age, race, gender, serum creatinine, urea and
albumin values
• Modified formula eliminates urea and albumin
• However underestimated eGFR when ≥ 60mL/min/1.73m2
66.
66
CKD-EPI Creatinine
• Developedin 2009 by the Chronic Kidney Disease Epidemiology
Collaboration (CKD-EPI)
• Does not require weight
• Developed against standardized reference assay for creatinine
• Better estimate of GFR than MDRD
• Requires use of age, race and serum creatinine
• Modified formula in 2021 removed race
67.
67
CKD-EPI cystatin C/CKD-EPICreatinine-cystatin C
• Developed in 2012 by CKD-EPI
• Incorporates cystatin C to overcome or obviate limitations of
creatinine
72
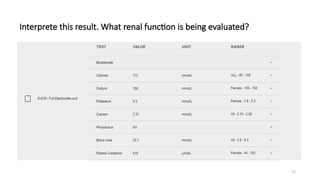
Calculate the eGFRusing Cockcroft-Gault and
CKD-EPI equations. What stage of CKD is this?
• 55 year old Nigerian male diagnosed to have diabetes mellitus 5 years
prior to admission. Weight 72kg; serum urea = 18.1mmol/L (2.5 – 6.4)
creatinine = 502µmol/L (50 - 106).
• For CKD-EPI Creatinine, demonstrate with on-line calculator
• https://www.mdcalc.com/calc/3939/ckd-epi-equations-glomerular-filt
ration-rate-gfr
73.
73
Review of learningobjectives…
• To appreciate the functional anatomy of the kidneys
• To understand the physiological roles of the kidneys
• To understand the categories of tests of renal function including tests
of glomerular and tubular function
• To appreciate the application of renal function tests in clinical practice
75
Conclusion…
• The kidneysare vital organs which play a myriad of clinical functions
• Defects in normal function of the kidneys have debilitating effects
• Kidney disease is quite common, being a complication of many prevalent non-communicable and
communicable diseases i.e diabetes mellitus, hypertension, sepsis/infections, drugs and toxins etc
• Laboratory investigation of kidney function requires comprehensive understanding of renal physiology
• Assessment of glomerular function is an invaluable index of overall kidney function through GFR and
clearance studies
• Understanding categories of tests of kidney function will guide clinicians in prompt and appropriate
management of kidney disease
KEY
MESSAGES
76.
76
Pre-test 1…
Which ofthe following is NOT regarded as a function of the kidney?
A. Fluid balance
B. Synthesis of thrombopoitein
C. Excretion of acid
D. Urine formation
E. Clearance
77.
77
Pre-test 2…
Which ofthe following is most accurate in assessing glomerular
function?
A. Creatinine
B. Cystatin C
C. Para-amino hippuric acid
D. Inulin
E. Iohexol
78.
78
Pre-test 3…
Which ofthe following kidney functions can be inferred from plasma
Calcium assay?
A. Storage function
B. Endocrine function
C. Synthetic function
D. Excretory function
E. Regulatory function
79.
79
Pre-test 4…
‘Electrolyte/urea/creatinine’ isone of the commonly requested
biochemical investigations. What category of kidney function tests can
it be classified?
A. Homeostatic function
B. Synthetic function
C. Excretory function
D. Homeostatic and synthetic function
E. Homeostatic and excretory function
80.
80
References
• Tietz textbookof Clinical Chemistry and Molecular diagnostics
• Comprehensive clinical nephrology
• Wikipedia
• Encyclopaedia Britannica
• www.researchgate.net
#18 GBM – Glomerular basement membrane
kDa – kilodalton
Mesangial cells – have contractile properties acting like smooth muscle cells in regulation of renal blood flow
#22 The thick ascending limb of the LOH is also referred to as the diluting segment
*Single osmotic effect vs countercurrent multiplication*
#23 This medullary concentration gradient is important in concentration of urine. Urea reabsorption and active efflux of Na, Cl and K contribute to this gradient
Individuals with psychogenic polydipsia abolish the formation of this concentration gradient and thus present with polyuria.
The thick ascending limb of the LOH is impermeable to urea. The collecting duct however has active UT-A1 and UT-A3 channels which result in active reabsorption of urea. This urea is recycled into the nephron at the thin descending and ascending limbs which are permeable to urea. The UT channels are influenced by ADH.
#25 Equilibration of the hypertonic interstitium with the isotonic capillary blood does not occur in the renal medulla despite the osmotic gradient
The U-shaped arrangement of vasa recta supplying the renal medulla ensures that solute entry and water loss in the descending vasa recta are offset by solute
loss and water entry in the ascending vasa recta.
This process is entirely passive and is referred to as the Countercurrent exchanger
#29 Collecting ducts empty into the minor and major calyces and subsequently into the renal pelvis and ultimately through the ureters to the urinary bladder and urethra for excretion
#39 In pathological states, the liver diverts ammonia from Urea synthesis into generation of glutamine which is utilized by the kidneys to generate ammonium ion
The Glutamine is hydrolysed in the kidneys by glutaminase to form glutamate and subsequently α-ketoglutarate and ammonium ion which then dissociates into NH3 and H+ acting as a urinary buffer
#47 R – Risk
I – Injury
F – Failure
L – Loss
E – End stage kidney disease
AKIN – Acute kidney injury network
CKD-EPI – Chronic kidney disease epidemiological consortium
KDIGO – Kidney disease improving global outcomes
#48 Inulin- polymer of fructose, continuous infusion – ‘Gold standard’
#50 Inulin – carbohydrate polymer of fructose; closed to ideal marker for clearance
#52 51Cr-EDTA is widely available in Europe but not available in
United States
#54 Creatine is synthesized in kidney, liver and pancreas from arginine and glycine via transamidation (forming guanidinoacetic acid) and methylation steps
#56 Positive association of Cystatin C with DM, cigarette smoking, CRP and WCC; inverse relationship with albumin
Method of assay – immunmetric e.g. particle-enhanced turbidimetric or nephelometric immune assay (PETIA or PENIA), ELISA
Traceability – ERM-DA 471/IFCC cystatin C in human serum developed by IFCC and listed in JCTLM database
Reference interval young adults (23 – 50yrs) = 0.6 – 1.1mg/L
#58 Treatment with cortisol results in protein breakdown
#63 Traceability of creatinine assay was not defined


![64
Cockcroft-Gault equation
• Formula: males…
[(140 - age) x weight x 1.23]/serum creatinine (in µmol/L)
OR [(140 - age) x weight/72 x serum creatinine (in mg/dL)]
• Multiply by a factor of 0.85 in females](https://image.slidesharecdn.com/renalfunctionandtestsofrenalfunction3-251126231141-10a587fb/85/Renal-function-and-tests-of-renal-function-3-pptx-64-320.jpg)


































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













