Downloaded 420 times




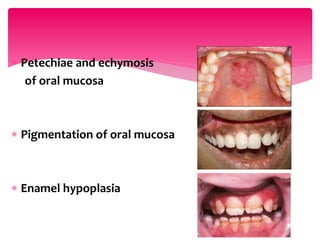





















This document discusses medical emergencies related to renal disorders and their oral manifestations. It covers various renal diseases including renal failure, glomerular diseases, and end stage renal disease. For patients with impaired renal function, oral manifestations can include xerostomia, parotitis, pigmentation, enamel hypoplasia, and candidiasis. Management of dental treatment for these patients requires consulting their physician, carefully monitoring blood pressure and drug dosages, and preventing infections. Special considerations are outlined for patients undergoing dialysis, renal transplants, or who have received a transplant.























































































