Downloaded 23 times

![II. Description of Agency Setting
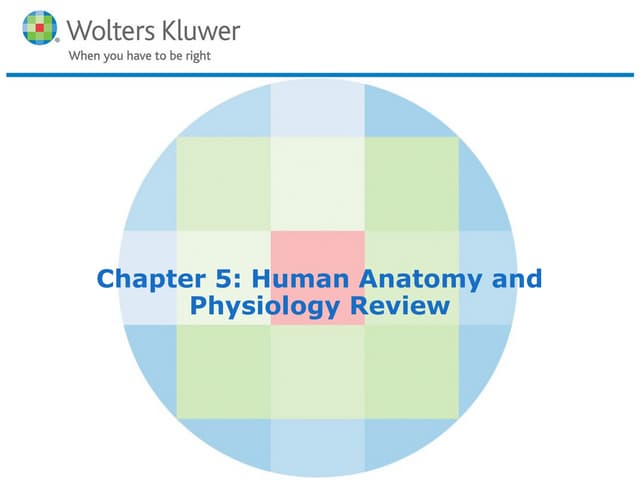
a. Therapeutic Recreation Model
The interdisciplinary clinical team at ResCare Premier Texas (RCP Texas) is quite
small. It includes four clinicians – one each in the specialties of physical,
occupational, speech-language and cognitive, and recreation therapies – and a
Clinical Director. As such, the therapists work together closely to develop, evaluate,
and modify treatment plans for individual participants and to execute those plans in
a consistent way. Out of obligation to provide quality, cohesive services as much as
out of proximity, then, these clinicians share a philosophy of treatment provision
that crosses the lines between specialties and inform practice perhaps even more so
than any discipline-specific model.
That shared interdisciplinary philosophy of service provision is one that emphasizes
consistency and positivity in focusing on the positive progress being made by
participants towards goals in which they are personally invested. As far as academic
models are concerned, it is most closely embodied in the Nurtured Heart Approach
(NHA) developed by Howard Glasser. While this service provision philosophy was
developed by Glasser as a strategy for parents and professionals working with
“intense” children, its core principles are readily applicable to “intense” adults with
TBI who exhibit challenging behaviors similar to those of the youth with ADHD and
ODD with whom Glasser was working. Those core principles include “refusing to
energive negative behavior,” “relentlessly energiz[ing] the positive,” and
“maintain[ing] total clarity about rules that demonstrate fair & consistent
boundaries.” The therapeutic philosophy surrounding the application of these
principles is one that is participant-centered and uses positivity rather than
punishment to achieve desired outcomes. (Children’s Success Foundation, 2015)
The therapeutic recreation model that fits most readily into the larger
interdisciplinary service provision philosophy is Dattilo, Kleiber, and Williams’ Self-
Determination and Enjoyment Enhancement model. This model is participant-
centered, emphasizing the need “to set the stage for people to enjoy themselves” by
“teaching [them], regardless of the . . . degree of disabilitity, to create environments
conduce to enjoyment” (p. 260). It is also readily applied in a community-based
setting that focuses on community resource education and skill acquisition through
active leisure participation – RCP Texas’ CTRS would readily agree with Dattilo,
Kleiber, and Williams’ suggest that progress towards desired outcomes and
increased independence occurs most readily “when people are encouraged and
supported to become aware of themselves in leisure contexts, make decisions and
choices, communicate their preferences, . . . set goals, . . . focus on internal standards,
emphasize inherent rewards, listen to informative feedback, and become aware of
their interests” (p. 262). Further evidence of the application of this model
throughout the therapeutic recreation process at RCP Texas will be seen throughout
this outline, particularly in that the philosophy of achieving functional
improvements through empowering participants to establish patterns of](https://image.slidesharecdn.com/casestudy-170119233428/85/REC-5338-Case-Study-2-320.jpg)

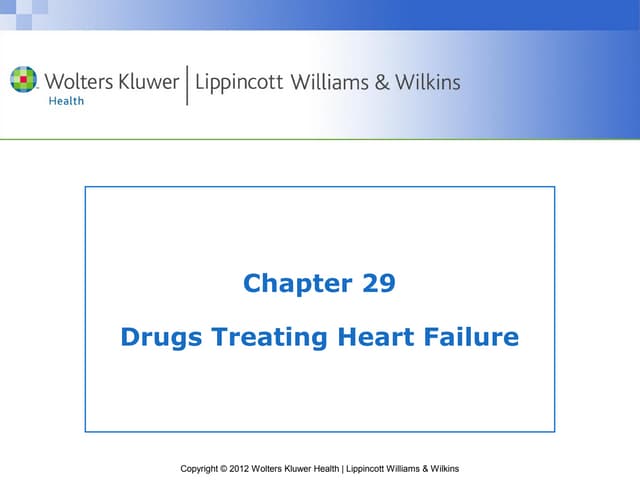
![attention deficit, divalproex for depression, and Seroquel for depression and
paranoia.
Participant lived in his parents’ home throughout his childhood with varying levels
of support and successfully completed secondary school through his local public
school system’s oral/deaf program. Upon graduation, participant moved out of his
parents’ home but had limited success living independently largely due to marijuana
abuse. Participant had both social and legal issues related to his marijuana abuse,
and it is suspected that he was involved in selling and/or distributing marijuana.
Upon being asked to leave a TBI-specific assisted living program due to issues
related to his marijuana abuse, participant was admitted to RCP Texas by his
parents and legal guardian.
At time of admission to RCP Texas, participant’s overall functional level was Level 7
on the Rancho Los Amigos scale, as he required minimal assistance for daily living
skills. Specifically, participant required moderate assistance related to behavioral
function and minimal assistance related to cognitive and communicative function,
but functioned independently related to gross and fine motor skills. Deficits
included lack of self-awareness, grandiose thinking, tendency to isolate, paranoid
thinking, trouble with budgeting and money management, and difficulty taking
responsibility. History of marijuana abuse was also viewed as a barrier. In order to
address the identified impairments, an interdisciplinary treatment plan was
developed to include recreation therapy, speech/cognitive therapy, individual
counseling and substance abuse treatment, group-based social and behavior skills
therapies, and community reintegration.
Participant is expected to reach Level 9 on the Rancho Los Amigos Scale and
establish a level of functional independence, requiring only supervision level
assistance upon request. Expected duration of services is six months or more.
Participant and legal guardian plan for discharge to an apartment in San Marcos
with limited supervisory level support provided by ResCare Premier Texas’
Independent Community Living program.
b. Diagnostic Criteria and Functioning Characteristics of Traumatic Brain Injury
The majority of ResCare Premier Texas’ participants, including the studied
participant, have been diagnosed with traumatic brain injury (TBI) of moderate to
severe classification. A TBI is defined, simply, as a “disrupt[ion] of the normal
function of the brain” caused by “a bump, blow, or jolt to the head or a penetrating
head injury” (Centers for Disease Control and Prevention, January 2016). As
prognosis and functioning characteristics of TBI participants varies widely, the
more telling factor of a TBI diagnosis is the classification of severity of the injury.
That classification is based on the use of several different diagnostic tools. The most
prominent is the Glasgow Coma Scale, used to evaluate severity of TBI during the
initial stages of treatment; scoring is based on eye-opening, verbal, and motor
responses to stimulation. Individuals “with GCS scores of 3 to 8 are classified with a](https://image.slidesharecdn.com/casestudy-170119233428/85/REC-5338-Case-Study-4-320.jpg)

![participants’ premorbid leisure interests, determining whether those interests
have been developed into a healthy leisure lifestyle post-injury or, if not, what
barriers have prevented such a development, and discussing with the participant
how it might be possible to establish transferrable healthy leisure participation
patterns within the context of RCP Texas’ community-based residential
rehabilitation model.
This tool was used in this particular case as it is the tool used in all recreation
therapy assessments for new admissions to RCP Texas. While there is no validity
or reliability information about this non-standardized tool, the usefulness of the
information gathered is ensured by the simple fact that the tool was developed
by the CTRS specifically for the purpose of informing therapeutic recreation
practice within the context of RCP Texas’ rehabilitation model. As the primary
goal of recreation therapy at RCP Texas is to assist participants in establishing
healthy leisure lifestyles within the context of RCP Texas that can then be
transferred to post-discharge settings, an assessment focusing on participant’s
leisure interests addressing barriers to participation is sufficiently informative.
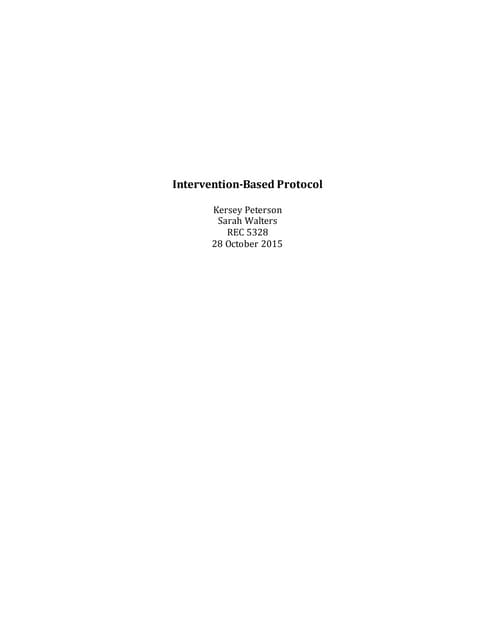
2. Assessment of the Studied Participant
The studied participant’s Recreation Therapy Assessment summary read:
[Participant] was outside with other participants during an arts and crafts
activity. [He] was sitting off towards the back of the group and had not
participated. [He] was introduced to CTRS by a Team Senior. [He] made eye
contact and reached his hand out for a handshake. CTRS noted appropriate eye
contact and handshake pressure. CTRS invited [participant] into the activity room
and he chose a seat next to CTRS at the table. [He] expressed he felt his anxiety
levels were high, however, he did not physically display an extreme level of anxiety
during his assessment. [He] stared off low and to his right for most of the
discussion, only making eye contact momentarily while he was speaking or if he did
not understand a question asked by CTRS. [He] was courteous and polite during the
assessment. At one point, [he] caught himself before using a curse word AEB
stopping mid-word, covering his mouth, and stating, “I’m sorry” before selecting
another word.
[He] talked about what he used and to and still likes to do in regards to recreation
and leisure. His stated interests include running, hiking, exploring, shopping, going
to the gym, photo editing, music making, dirt biking, going to the library, festivals,
acting classes, playing and researching on the internet, and using programming
apps. [He] expressed wanting to “make a gangster movie” and become a movie
star. He expressed enjoying leisure both only and with friends, though “only ones he
can trust.” He identified only two barriers to leisure – being at RCP and being
unable to leave the program facility. He was able to identify benefits of leisure
participant and, when asked how often he participates in leisure, responded, “It
depends.”](https://image.slidesharecdn.com/casestudy-170119233428/85/REC-5338-Case-Study-6-320.jpg)
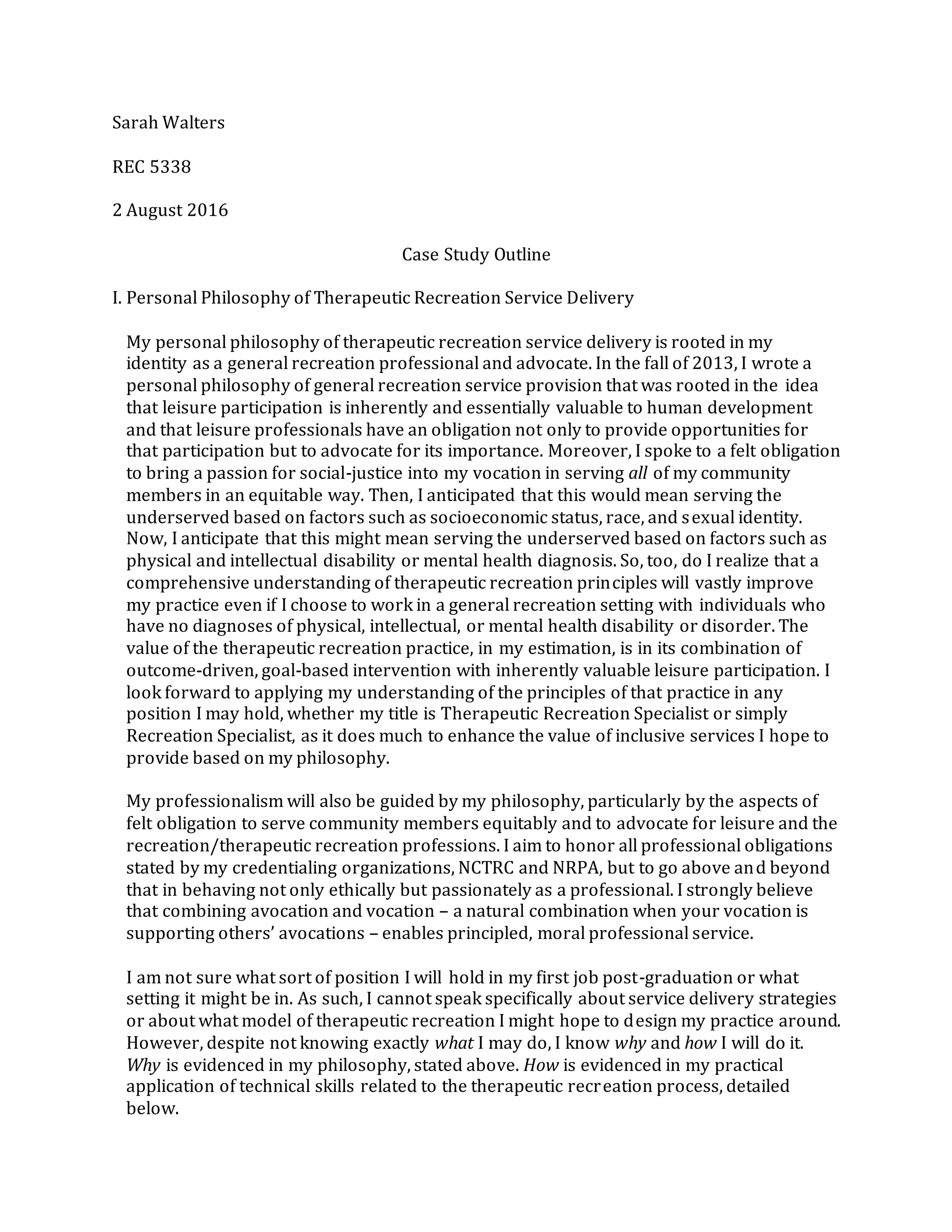
![[Participant] stated that he was confused about why he was at RCP Texas and
continued to make comments about “weed” possibly being the reason. [He] spoke of
“weed” several times, stating that he is not addicted, that it will be legalized, and
that he doesn’t understand why people think “weed” is “bad.” He discussed a friend
he’d had and that he wanted to help that friend “help the organization grow” and
“build up customers,” implying some sort of involvement in selling/distributing
“weed.”
When asked about his impairments and desire to make improvements,
[participant] expressed he felt he should be in an apartment where staff come by
only once a day and help him pay bills, get out into the community, and get to
various activities. He did state that he “has problems focusing.” Finally, he
expressed that he thinks he is “wasting [his] time in this place.”
CTRS observed attention deficit AEB [participant]’s ease of distraction by any noise
or motion and request to go to “a more private place.” CTRS observed sporadic
thinking and cyclic thought patterns, as well as a tendency to describe moments in
time rather than general ideas or complete thoughts. During the interview, CTRS
needed to ask [him] to repeat himself several times due to low speech volume and
observed continuous wringing or motioning of hands.
CTRS recommends individual recreation therapy services 1 time per week for 1
hour each for a minimum of 90 days after admission. CTRS will provide
individualized support as needed and notification of community opportunities as
appropriate.
b. Therapeutic Plan Recommended for Studied Participant
Current recreation therapy treatment goals and objectives for the studied
participant are:
1. [Participant] will identify and participate in healthy leisure outlets of interest in
order to create leisure stability.
a. During each weekly individual recreation therapy session, [participant] will
develop a plan for the subsequent session including activity, location, and
schedule with minimal assistance.
b. [Participant] will independently arrange transportation and supervision for a
weekly visit to the San Marcos Library.
c. [Participant] will acquire a tablet computer during this service period.
2. [Participant] will consistently demonstrate suitable social skills in all
interactions.](https://image.slidesharecdn.com/casestudy-170119233428/85/REC-5338-Case-Study-7-320.jpg)
![a. During each weekly individual recreation therapy session, [participant] will
provide appropriate, on-topic responses to questions from CTRS and TR
Intern on 90% of opportunities with minimal assistance.
b. [Participant] will attend weekly “Stress Management” group therapy sessions
on 6 out of 8 opportunities.
c. During individual recreation therapy sessions involving community outings,
[participant] will appropriately initiate and complete interactions with
customer service representatives on 100% of opportunities with no
assistance.
The participant’s goals were developed based on information gathered during the
initial assessment, as well as on discussions with the treatment team and with the
participant. The first goal was selected based on participant’s history of unhealthy
leisure participation related to marijuana abuse and the need to establish
alternative, healthy leisure patterns. The second goal was selected based on an
historic tendency to isolate, participant’s implication that he had struggled to
maintain healthy relationships, and CTRS’ observation of social anxiety and
generally poor social skills during assessment interview. These goals were also
selected because the treatment team determined that developing alternatives to
marijuana use and improving social skills would be primary requirements for
discharge.
While the general concept of each objective has remained consistent throughout
participant’s time at RCP Texas, the degree and intensity of each objective has been
revised periodically based on his progress. Like the goals which they fall under,
these objectives are also rooted in information gathered during the initial
assessment.
Current objectives under goal one are based on the participant’s expressed leisure
interests and the expectation that he be able to independently identify and arrange
opportunities for participating in those activities of interest before being
discharged. The first objective, specifically, delineates the fulfillment of that
expectation quite generally. The second and third objectives are related to
particular activities of interest.
Similarly, current objectives under the second goal are based on the expectation that
the participant be able to communicate appropriately in all settings before being
discharged. The first objective considers a particular social skill addressed in the
context of individual therapy as it is most relevant to and measurable in one-on-one
or small group conversations involved the CTRS directly. The second objective is
related to the participant’s involvement in group-based social skills therapy and the
expectation that he participates consistently in order to receive the desired benefits.
The third objective addresses a need to improve confidence in interactions with](https://image.slidesharecdn.com/casestudy-170119233428/85/REC-5338-Case-Study-8-320.jpg)

![pattern of significant improvements to engagement in leisure activities and
degree of social involvement related to participation in those activities. Brown,
Gordon, and Spielman (2003) found that participants in their studied community
integration intervention saw positive outcomes related to frequency of
participation in leisure activities and time spent participating in leisure activities
and to related functions necessary for recreation participation such as
independently accessing transportation and accessing places where participants
could meet people with whom they could participate in leisure. Fleming and
colleagues (2011) found that the most essential benefit of leisure-based
community integration was that it enabled participants to continue recreation
participation, and therefore continue to receive the benefits of that participation,
while in rehabilitation facilities, a finding related concisely in their conclusion
statement:
“Leisure participation of individuals with ABI significantly decreased during
both inpatient and outpatient rehabilitation. This indicates that re-
engagement in age-appropriate and relevant leisure activities needs to be
addressed during the rehabilitation phase to improve participation and
future outcomes in this domain. However, this does not imply that the
desired goal is to improve frequency and activity participation to pre-morbid
levels; rather the desired longer term outcome is satisfaction with leisure
participation.” (p. 816).
This finding counteracts the commonly held belief that “diversionary” recreation
participation, or participation for the sake of participation, has limited
therapeutic benefits for long-term rehabilitation participants. On the contrary, it
is essential for achieving those therapeutic benefits, particularly when desired
benefits are related to establishing or re-establishing a healthy leisure lifestyle,
as in the case of the studied participant.
3. Relating the Studied Intervention to Desired Outcomes
As mentioned previously, the intervention strategy used was effective in that it
allowed progress towards both treatment goals through practical experience
and consistent but subtle therapeutic processing of that experience. One
example of such progress was seen in an individual recreation therapy session
summarized in a progress note:
Due to a scheduling conflict, a trip to see The Purge: Election Year at Alamo
Drafthouse was rescheduled from late June. [Participant]’s hearing aid battery died
just before departing for the theatre, but he requested that we still see the movie.
He explained that he “enjoys being deaf” and still engaged CTRS and Intern in
conversation, teaching us bits of ASL to supplement lip-reading. Upon arriving at
the theatre, [participant] appropriately interacted with ticket booth staff and
requested an accommodation while completing the transaction. He chose closed](https://image.slidesharecdn.com/casestudy-170119233428/85/REC-5338-Case-Study-10-320.jpg)
![captioning glasses over sound amplifying headphones. On the drive back from the
theatre, [participant] initiated a discussion about the relevance of the movie’s plot
to current events and respected requests not to discuss politics on too personal a
level. Participant not only responded appropriately to questions when asked but
followed responses with return questions to keep our conversation flowing.
This session’s experience with planning and participating in a healthy leisure
activity, practicing social skills, and processing during casual conversation
contributed to the achievement of several objectives, also summarized in the
quoted progress note:
1a. During each weekly individual recreation therapy session, [participant]
will develop a plan for the subsequent session including activity, location,
and schedule with minimal assistance.
Status: Achieved/Continue. [Participant] independently requested outings to
movies at Starplex and Alamo Drafthouse, the batting cage, Half Price Books, and
Dairy Queen. His naming of specific locations indicated progress towards
identifying not only an activity but a specific community resource for participating
in that activity. On each occasion, he coordinated scheduling with CTRS and TR
Intern successfully. [Participant] required minimal assistance to search movie
times and to find an indoor batting cage in the area.
2a. During each weekly individual recreation therapy session, [participant]
will provide appropriate, on-topic responses to questions from CTRS and TR
Intern on 90% of opportunities with minimal assistance.
Status: Achieved/Continue. [Participant] provided appropriate, on-topic responses
on 90% of occasions during this service period. During one session, [participant]
became visibly distressed during a conversation and was unable to provide
clarifying information after telling a wandering, incomplete story. However, during
other sessions, participant led engaging discussions, responding to and asking
questions appropriately to move conversations along.
2c. During individual recreation therapy sessions involving community
outings, [participant] will appropriately initiate and complete interactions
with customer service representatives on 100% of opportunities with no
assistance.
Status: In Progress/Continue. [Participant] appropriately interacted with
customer service representatives at Dairy Queen and at the movie theatres, but
required prompting from CTRS to initiate interactions.
The participant may have benefitted from identifying leisure activity
opportunities and planning them hypothetically in a facility-based leisure
awareness intervention, and could have developed social skills in interactions
with CTRS and TR Intern during those facility-based sessions. However, the
benefits seem to be multiplied significantly by the real-world experience of](https://image.slidesharecdn.com/casestudy-170119233428/85/REC-5338-Case-Study-11-320.jpg)


![Participant: Program: TBP South
DOB: Service Period: July 2016
Diagnosis: TBI Physician: J. Wesley Wallis,MD
DOI: 6/1998 Therapist: Ashley Franks,CTRS
Sarah Walters, TR Intern
Impairments: Hearingimpairment, lack of self-awareness,grandiosethinking,tendency to isolate,paranoid
thinking,trouble with budgeting and money management, difficulty takingresponsibility,substanceabuse
Subjective/Objective: [Participant] received individual recreation therapy services 5 times this serviceperiod.
7/8/2016:Due to a schedulingconflict,a trip to see The Purge: Election Year at Alamo Drafthousewas rescheduled
from late June. [Participant]’s hearingaid battery died justbefore departingfor the theatre, but he requested that
we still seethe movie. He explained that he “enjoys being deaf” and still engaged CTRS and Intern in conversation,
teaching us bits of ASL to supplement lip-reading.Upon arrivingatthe theatre, [participant] requested an
accommodation and chose closed captioningglasses over sound amplifyingheadphones.On the drive back from
the theatre, [participant] initiated a discussion aboutthe relevance of the movie’s plot to current events and
respected requests not to discusspoliticson too personal a level. Participantnotonly responded appropriately to
questions when asked but followed responses with return questions to keep our conversation flowing.
7/11/2016:Visited the San Marcos Library to exchange DVDs and use WiFi.[Participant] exhibited safeinternet use
and interacted appropriately with the librarian atthe front desk. Duringthe drive back to the program,
[participant] explained to CTRS and TR Intern that he thought he had made significantprogress sincearrivingat
ResCare but acknowledged that he still needed help before he’d be ready to livein an apartment. CTRS and TR
Intern agreed and encouraged [participant] to discuss whatprogress he still wanted to make.
7/18/2016:Visited Dairy Queen and Half PriceBooks. With prompting from CTRS to initiate,[Participant]
appropriately completed transaction atDairy Queen. At Half PriceBooks, [he] independently held to an agreed
upon 20-minute time limitand found CTRS and TR Intern to remind us it was time to go. Duringthe return trip to
the program, something in our conversation reminded [participant] of an estranged friend, prompting a
disconnected and incomplete story about their fallingout.He was visibly shaken by the conversation and was
unableto clarify or reflectupon details of the story when asked by CTRS. His mood remained low upon returning
to the programdespite havingexpressed several times that he was “havinga great day” prior to his tellingthe
story.
7/23/16: Visited the Austin Batting Cages. [Participant] independently gathered a bat and helmet upon arrival and
spent 30 minutes batting, pickingup the balls to reload the pitchingmachineas necessary with the help of CTRS
and TR Intern. After leavingthe cages,[participant] requested that we stop at Whataburger to eat but changed his
mind when we passed a Wendy’s. Whileeating,a TV showingthe news seemed to prompt himto ask CTRS and TR
Intern about political views,butrespectfully changed the topic when both expressed that they weren’t
comfortable with the question.
Assessment: [Participant]’s progress duringJuly 2016 serviceperiod was as follows:
1a. During each weekly individual recreation therapy session, [participant] will develop a plan for the
subsequent session including activity, location, and schedule with minimal assistance.
Status: Achieved/Continue. [Participant] independently requested outings to several movies,the batting cage,
Half PriceBooks, and Dairy Queen. His naming of specific locations indicated progress towards identifyingnot
only an activity buta community resource for participatingin thatactivity.On each occasion,hecoordinated
schedulingwith CTRS and TR Intern successfully.[Participant] required minimal assistanceto search movie
times and to find an indoor battingcage in the area.](https://image.slidesharecdn.com/casestudy-170119233428/85/REC-5338-Case-Study-14-320.jpg)
![1b. [Participant] will independently arrange transportation and supervision for one visit to the San Marcos
Library per week of this service period.
Status: In Progress/Continue.[Participant] successfully arranged transportation and supervision for trips to the
library in 3 outof 4 weeks duringthis serviceperiod. He was unableto do so in the final week of the service
period due to a situation thatprevented program staff from providingtransportation and supervision.
1c. [Participant] will acquire a tablet computer during this service period.
Status: Achieved/Revise. [Participant] successfully budgeted for a tablet computer and arranged a visitto Best
Buy to purchasethe tablet.
2a. During each weekly individual recreation therapy session, [participant] will provide appropriate, on-topic
responses to questions from CTRS and TR Intern on 90% of opportunities with minimal assistance.
Status: Achieved/Continue. [Participant] provided appropriate,on-topic responses on 90% of occasions during
this serviceperiod. During one session,[participant] becamevisibly distressed duringa conversation and was
unableto provideclarifyinginformation after tellinga wandering,incomplete story. However, duringseveral
other sessions,participant led engaging discussions,respondingto and askingquestions appropriately to move
conversations along.
2b. [Participant] will attend weekly “Stress Management” group therapy sessions on 2 out of 3 opportunities
during the July service period.
Status: Achieved/Revise. [Participant] attended two of the three “Stress Management” sessions held in July,but
missed the final session atno faultof his own. He later apologized for missingthe fi nal session and explained
that his staff were under the impression thatthe group had ended the previous week.
2c. During individual recreation therapy sessions involving community outings, [participant] will
appropriately initiate and complete interactions with customer service representatives on 100% of
opportunities with no assistance.
Status: In Progress/Continue.[Participant] appropriately interacted with customer servicerepresentatives at
Dairy Queen and at the movie theatre, but required prompting from CTRS to initiateinteractions.
Plan: Continue individual recreation therapy services.[Participant] will beencouraged to attend “Healthy
Relationships”group beginningAugust 10, 2016 for 8 weeks. Revised treatment objectives for the August 2016
serviceperiod include:
2b. [Participant] will attend weekly “Healthy Relationship” group therapy sessions on 3 out of 4
opportunities during the August service period.
1c. [Participant] will use his tablet computer to independently download and watch a movie.
Expected Duration of Recreation Therapy: Individual recreation therapy services to be provided through
December 2016.
Intensity of Recreation Therapy: 1 hour Individual
Intensity of Recreation Therapy: 1 hour Group
Frequency of Recreation Therapy: Individual recreation therapy services and group recreation therapy services 1
time per week each.
Summary: CTRS recommends [participant] continueto receive individual recreation therapy services 1 time per
week for 1 hour each session in order to continue progress on his treatment goal s and objectives.CTRS also
recommends that [participant] attend “Healthy Relationships”group beginningAugust 8, 2016 for 8 weeks. CTRS
will provideindividualized supportas needed and notify of community opportunities as appropriate.
_____________________________________________________ _____________
Sarah Walters, TR Intern Date](https://image.slidesharecdn.com/casestudy-170119233428/85/REC-5338-Case-Study-15-320.jpg)
![Participant: Program: Hutchison Place
DOB: Service Period: December 2016
Diagnosis: TBI Physician: J. Wesley Wallis,MD
DOI: 6/1998 Therapist: Ashley Franks,CTRS
Sarah Walters,TR Intern
Impairments: Hearingimpairment, lack of self-awareness,grandiosethinking,tendency to isolate,paranoid
thinking,trouble with budgeting and money management, difficulty takingresponsibility,substanceabuse
Subjective/Objective: [Participant] received individual recreation therapy services 3 times this serviceperiod.
12/5/16: Saw a theatre production put on by the Texas State drama program. When another patron was usinghis
cell phone duringthe performance, [participant] quietly pointed itout to CTRS who was then able to notify an
usher. After the performance, [participant] stated that he would liketo begin actingclasses oncehe left ResCare.
12/12/16:Observed an actingclassatBriteLites Studio in Austin. After the classwas over,[participant] initiated a
conversation with the instructor about his experience and actingphilosophy.[He] asked for information about
upcoming classes and pricing.
12/19/16:Visited the Sights and Sounds festival.Throughout the outing, [participant] reflected on progress made
whileat ResCare Premier and willingly engaged with CTRS in discussion aboutmaintainingthatprogress once he
moved to his apartment. [Participant] initiated conversation with couplestandingin linebehind us and shared an
appropriatelevel of information abouthimself and his situation when asked.
Assessment: [Participant]’s progress duringDecember 2016 serviceperiod was as follows:
1a. [Participant] will independently develop plans for weekly individual recreation therapy sessions including
activity, location, and schedule.
Status: Achieved/Discontinue. [Participant] independently planned an activity for each of his three individual
recreation therapy sessions duringthis period,identifyingthelocations and makingschedulingadjustments
with the CTRS as necessary.
1b. [Participant] will independently visit the San Marcos Library one time per week this service period.
Status: Achieved/Discontinue. [Participant] successfully used CARTS to travel to the library timeduringeach
week of this serviceperiod.He continues to consistently return movies on time and has had no problems with
inappropriateinternet use.
1c. [Participant] will independently budget for planned recreation activities using a web-based budgeting
application.
Status: Achieved/Discontinue. [Participant] successfully predicted costs of planned recreation activities and
spent no more than the predicted amount.
2a. During each weekly individual recreation therapy session, [participant] will provide appropriate, on-topic
responses to questions from CTRS on 100% of opportunities with no assistance.
Status: Achieved/Discontinue. [Participant] provided appropriate,on-topic responses on all occasionsduring
this serviceperiod. His turn-taking also continues to improve, as he consistently follows an appropriate
responsewith a return question.](https://image.slidesharecdn.com/casestudy-170119233428/85/REC-5338-Case-Study-16-320.jpg)
![2b. [Participant] will attend weekly “Community Living” group therapy sessions on 3 out of 3 occasions
during the December service period.
Status: Achieved/Discontinue. [Participant] attended 3 of the 3 “Community Living” sessionsheld in December
and actively participated in each session,frequently providingfeedback to questions of other participants.
2c. [Participant] will appropriately initiate conversation with a new conversation partner during at least one
individual recreation therapy session involving a community outing.
Status: Achieved/Discontinue. Whilewaitingin a lineat Sights and Sounds, [Participant] appropriately greeted
a couple standingbehind us and asked them whether they had ever attended the festival before.
Plan: Discontinuerecreation therapy services and dischargefromResCare Premier Texas .
Expected Duration of Recreation Therapy: Individual recreation therapy services to be discontinued.
Intensity of Recreation Therapy: Individual
Intensity of Recreation Therapy: Group
Frequency of Recreation Therapy: Recreation therapy services to be discontinued.
Summary: As he has met expectations for dischargeby achievingall goalsand therefore completed his treatment
plan,CTRS recommends [participant] bedischarged fromrecreation therapy services as well as fromResCare
Premier Texas’ Hutchison Placeprogram. CTRS concurs with the treatment team recommendation that
[participant] bedischarged to an apartment in San Marcos to liveindependently while continuingto receive
supervisory level supportas requested through ResCare Premier Texas’ Independent Community Livingprogram,
as well as the recommendation that this supportbe limited to weekly medical check-ins,monthly budgetary check-
ins,and infrequent transportation.CTRS also supports therecommendation that [he] continue to attend individual
counselingand substanceabusesessionsthrough his currentprovider but receive no other therapy services.
In regards to leisureparticipation specifically, CTRS recommends [participant] continueto use CARTS to
independently access thecommunity and maintain participation in community-based recreation activities such as
visitingthelibrary to borrow DVDs, runningat the Activity Center or Greenbelt, seeing movies at the Starplex
theatre, and attending local events. Participation in home-based leisureactivities such as usinghis computer to
make music,edit photos, and research interesting topics as well as workingon his moviescriptshould also be
maintained.CTRS also recommends [participant] establish participation in actingclasses or an actingclub.CTRS
sees no need for referral to continued recreation therapy services or other supportservices specific to leisure
participation.
_____________________________________________________ _____________
Sarah Walters, TR Intern Date](https://image.slidesharecdn.com/casestudy-170119233428/85/REC-5338-Case-Study-17-320.jpg)




The participant was assessed using a non-standardized assessment tool developed by the CTRS. The assessment gathered information on the participant's diagnosis, interests, and barriers to leisure participation. It found the participant enjoys activities like running, hiking, and music but identified being at the facility and inability to leave as barriers. The participant displayed some confusion about why he was at the facility and made comments implying past involvement with marijuana distribution. He expressed a desire to live independently with only once daily staff checks.