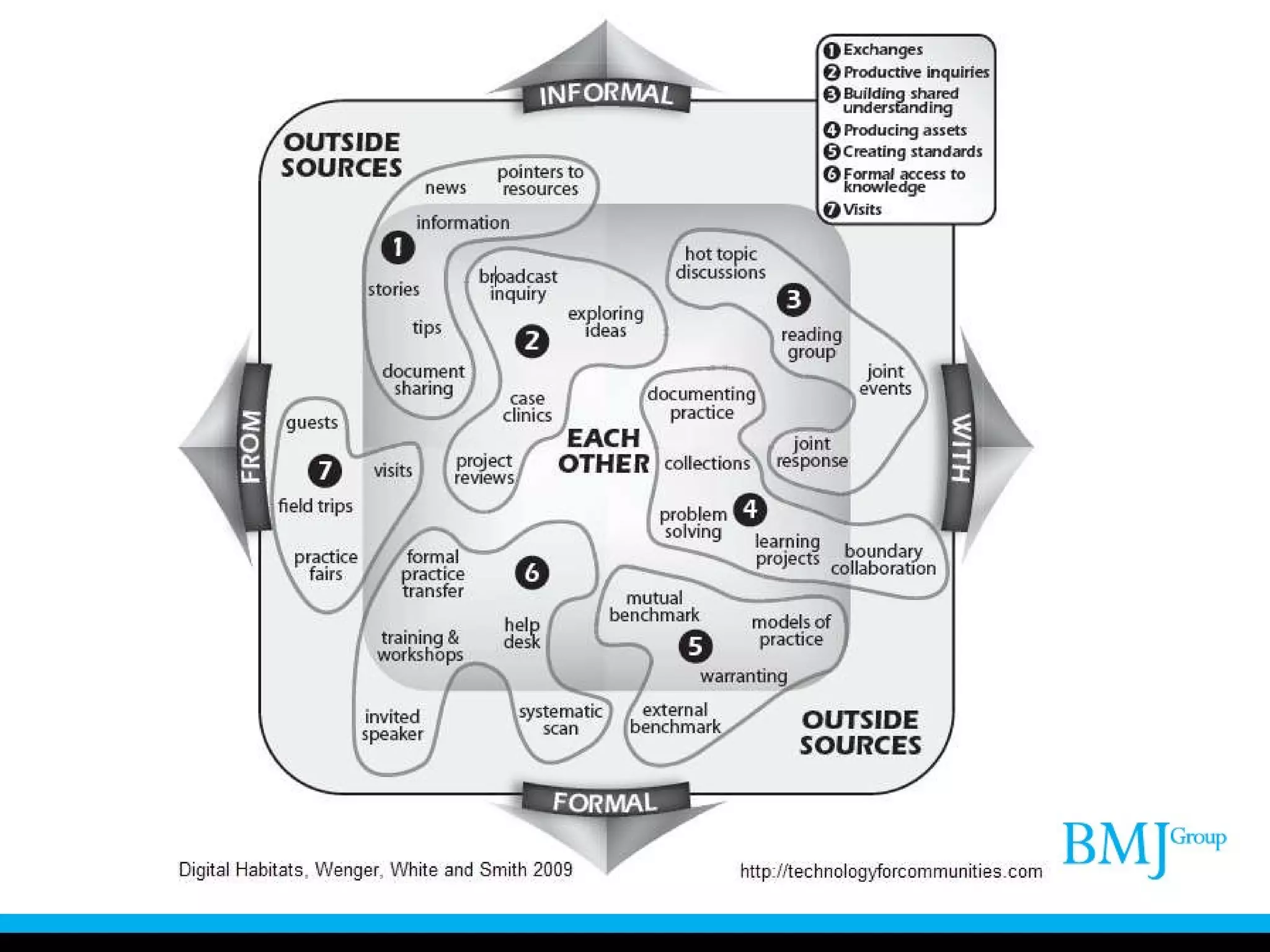
The document discusses a blended learning programme called the Diabetes Academy that was piloted in four countries to improve diabetes care among primary care physicians. It identified four key gaps through needs assessments and used a communities of practice framework. A formative evaluation found communities starting to form and some self-reported performance improvements. The programme demonstrated the complexity of educational interventions for performance improvement and the need for evaluation and participant motivation strategies.