Download to read offline

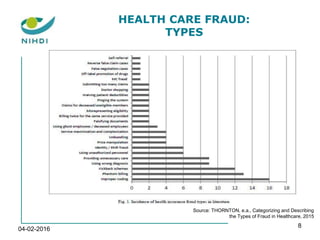


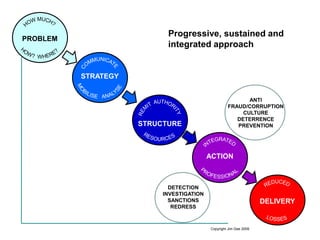





The document discusses healthcare fraud in Belgium, highlighting the increasing awareness and strategic efforts to combat it through a robust and integrated approach. It outlines various types of fraud, the roles of sickness funds and the National Institute for Health and Disability Insurance (NIHDI), and emphasizes the need for prevention, investigation, and enforcement measures. Additionally, it presents the importance of international cooperation and data availability to address inappropriate and low-value care in healthcare systems.
































































