Downloaded 146 times



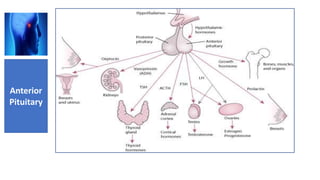
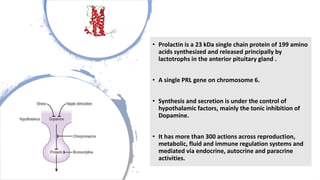



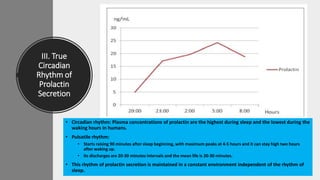


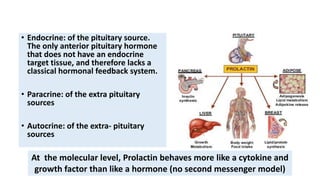














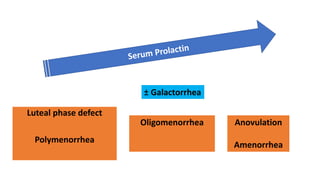













Prolactin is a unique hormone that has more than 300 functions across multiple body systems. It is produced primarily in the pituitary gland but also in other tissues. Prolactin levels have a circadian rhythm and are regulated by the hypothalamus. Abnormal prolactin levels can be caused by prolactinomas, drugs, or physiological states. Prolactinomas are benign pituitary tumors but macroadenomas larger than 1 cm require treatment. High or low prolactin impacts fertility in both males and females. Treatment involves lowering prolactin levels through dopamine agonists like bromocriptine or newer drugs.



































![Pituitary gland 2025 [Autosaved].cccpptx](https://cdn.slidesharecdn.com/ss_thumbnails/pituitarygland2025autosaved-250619094157-8c4103a0-thumbnail.jpg?width=640&height=640&fit=bounds)



















































