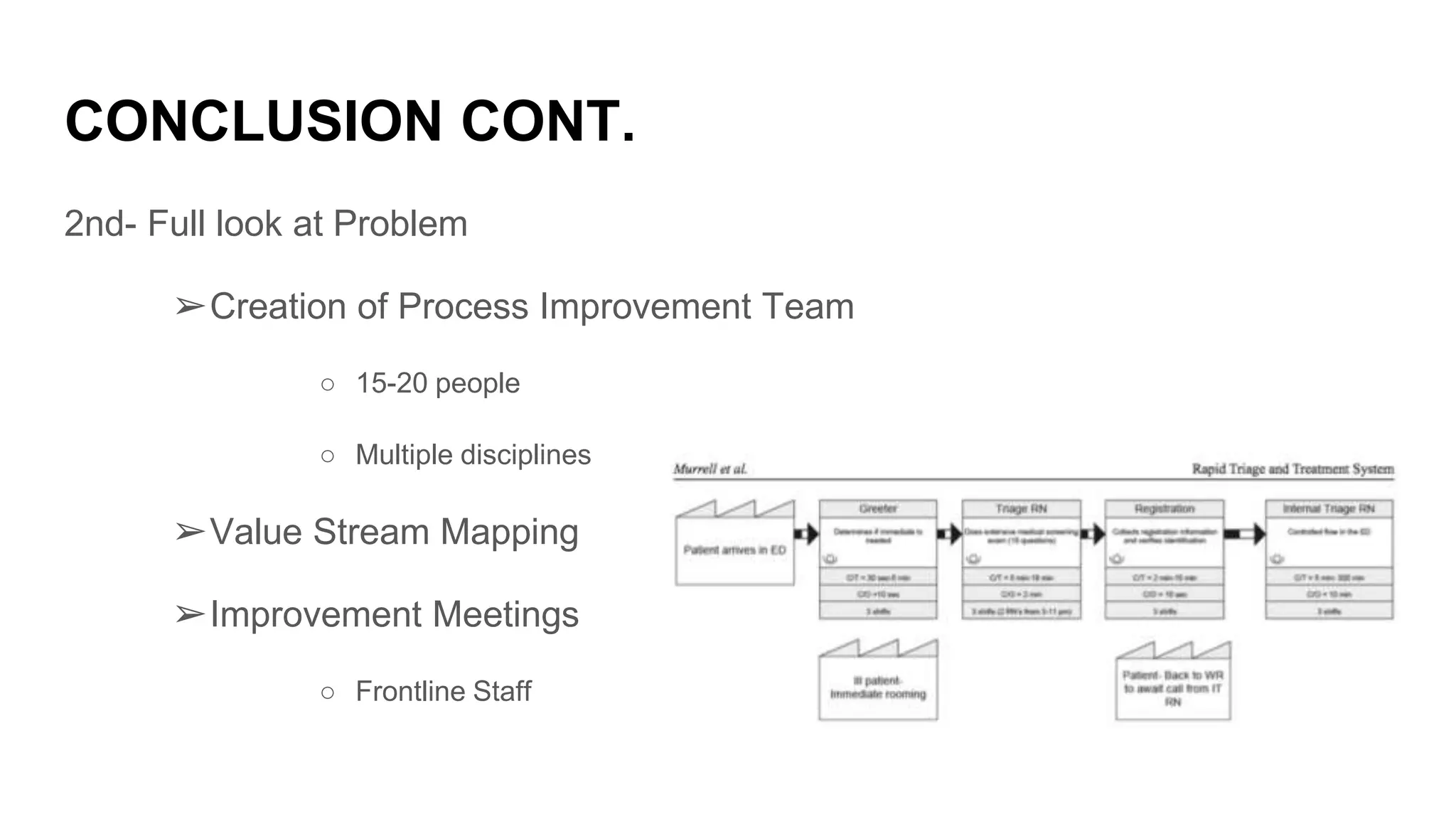
This document discusses strategies to improve patient flow in emergency departments. It notes that ED visits in the US have increased significantly in recent decades, leading to overcrowding issues. The purpose is to review literature on techniques to improve ED efficiency and identify gaps that lead to overcrowding. Some strategies discussed include implementing fast tracks to separate high and low acuity patients, using rapid triage and treatment areas, and applying lean manufacturing principles like continuous process improvement teams. The conclusion emphasizes that successful strategies require a safety culture, fully analyzing the problems, and slowly implementing changes while measuring outcomes.