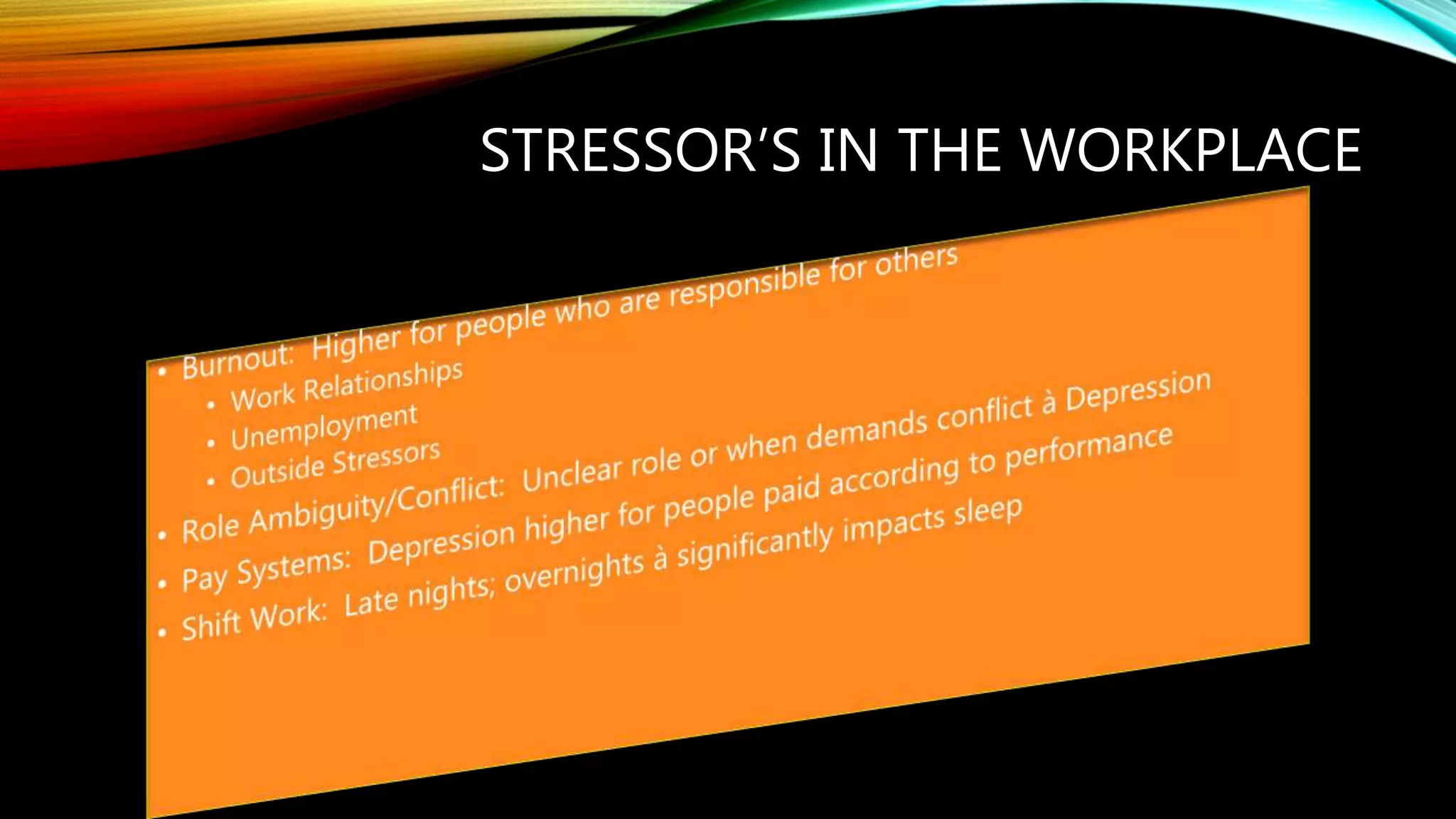
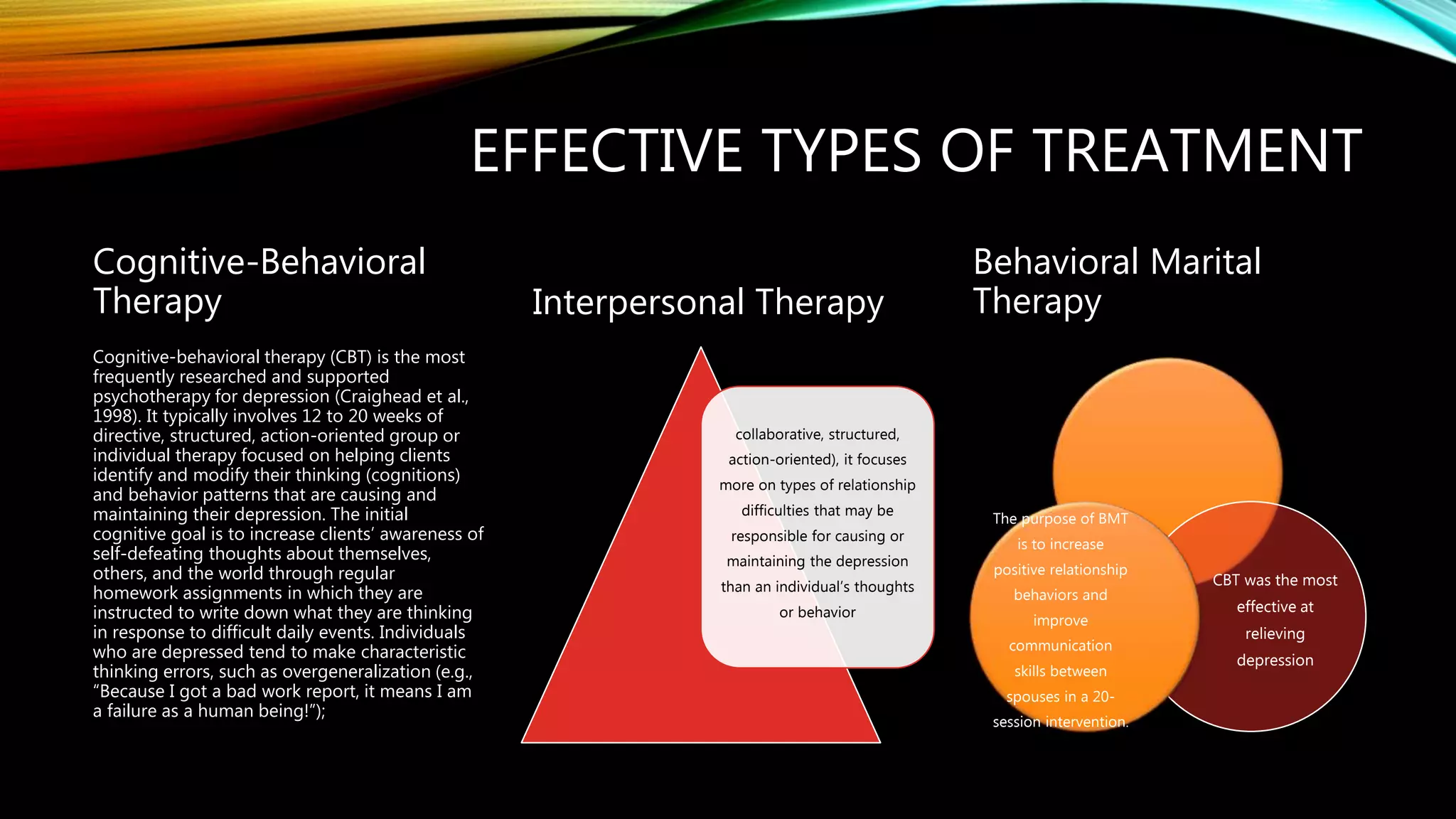
This document discusses depression, including its causes, symptoms, and treatments. It notes that depression can be diagnosed in several forms and have a variety of symptoms, including loss of pleasure, changes in appetite or sleep, low mood, and thoughts of death. Common treatments include cognitive behavioral therapy, antidepressants, and interpersonal therapy. The document also discusses challenges related to depression in the workplace, such as work stressors, and recommends that employers increase awareness and support for employee mental health issues.