* A 23-year-old pregnant woman with epilepsy was admitted to the hospital at 40 weeks of pregnancy. She has a history of epilepsy since 2012 and has been taking carbamazepine and clonazepam to control her seizures.
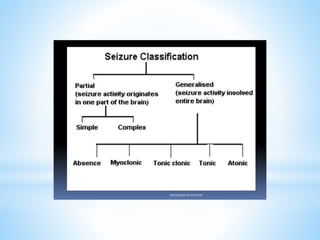
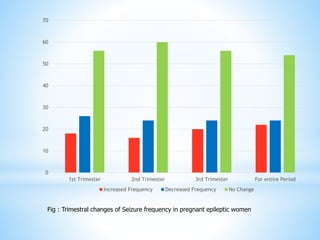
* Epilepsy is a chronic neurological disorder characterized by recurrent seizures. Pregnancy can impact seizure frequency in women with epilepsy, though most experience no change or a decrease. Antiepileptic drugs also carry risks of birth defects, developmental issues, or pregnancy complications.
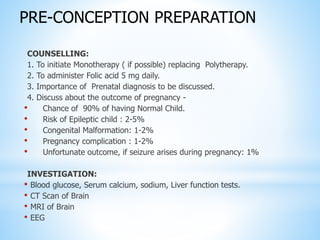
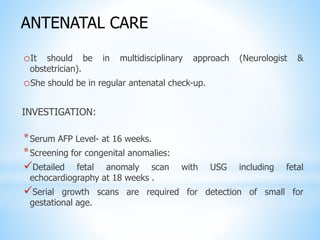
* Careful prenatal care including screening, continued medication, folic acid, and delivery in a hospital equipped to treat seizures is recommended to support healthy outcomes for both mother and baby.