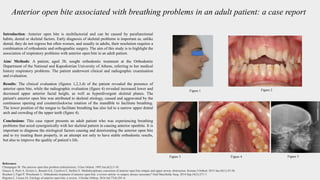
This case report describes an adult patient who presented with an anterior open bite that was associated with breathing problems. Clinical and radiographic examination revealed the open bite was due to skeletal factors including an increased lower anterior facial height and hyperdivergent skeletal planes. The patient's breathing problems acted synergistically with her skeletal pattern to cause and worsen the open bite over time as her mandible rotated counterclockwise to open and facilitate breathing. Treatment of the open bite would need to address both the skeletal and respiratory etiological factors.