Introduction
Kouchoukos, N., Blackstone,E., Hanley, F., Kirklin, J. 2013. Kirklin/Barratt-Boyes Cardiac Surgery Fourth Edition: PostinfarctionVentricular Septal Defect. Saunder
Elsevier. P446-459
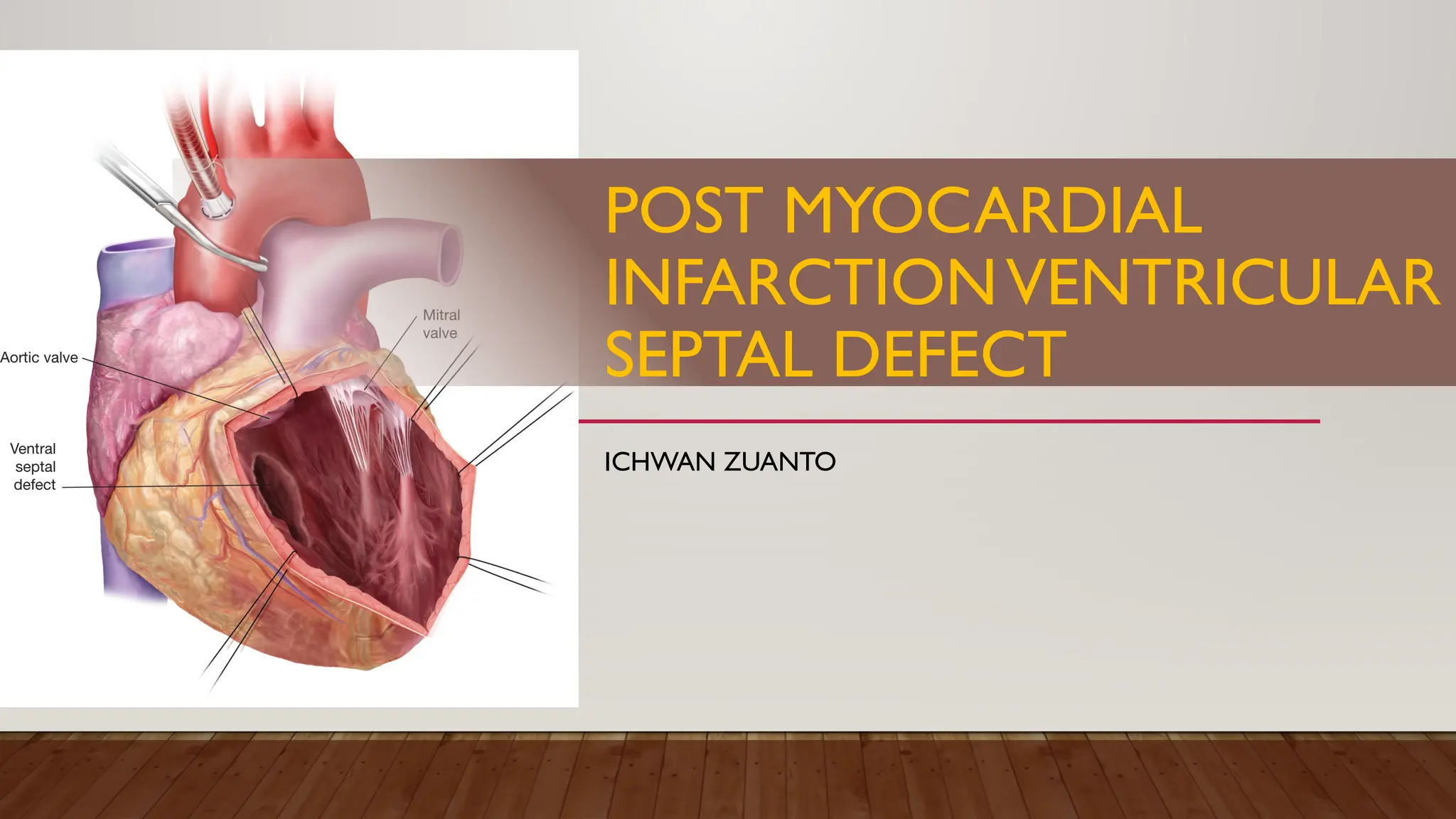
• Postinfarction ventricular septal defect is an opening in the ventricular septum resulting from
rupture of acutely infarcted myocardium
• VSD occurs in 1-2% of all acute MI, typically 3-5 days after onset of symptoms, can occur as early
as hours or as late as 2 weeks.
• Median age 72 years, higher incidence of hypertension and diabetes
3.
Introduction
• Area ofinfarction:
• 70% anterior
• 29% inferior
• 1% other cardiac zones
• Single vessel coronary disease was present in 50% of patients
• Survival was higher for anterior infarction (51%vs9%)
Kouchoukos, N., Blackstone, E., Hanley, F., Kirklin, J. 2013. Kirklin/Barratt-Boyes Cardiac Surgery Fourth Edition: PostinfarctionVentricular Septal Defect. Saunder
Elsevier. P446-459
4.
Risk Factors
• Women
•Anterior Infarction
• No previous history of angina/MI
• Hypertension
• Age > 60 yo
Kouchoukos, N., Blackstone, E., Hanley, F., Kirklin, J. 2013. Kirklin/Barratt-Boyes Cardiac Surgery Fourth Edition: PostinfarctionVentricular Septal Defect. Saunder
Elsevier. P446-459
5.
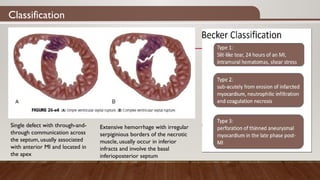
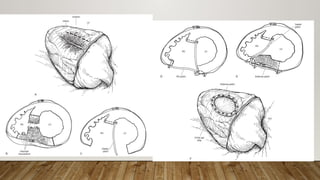
Classification
Single defect withthrough-and-
through communication across
the septum, usually associated
with anterior MI and located in
the apex
Extensive hemorrhage with irregular
serpiginious borders of the necrotic
muscle, usually occur in inferior
infracts and involve the basal
inferioposterior septum
6.
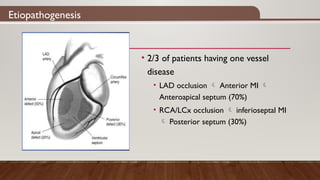
Etiopathogenesis
• 2/3 ofpatients having one vessel
disease
• LAD occlusion Anterior MI
Anteroapical septum (70%)
• RCA/LCx occlusion inferioseptal MI
Posterior septum (30%)
7.
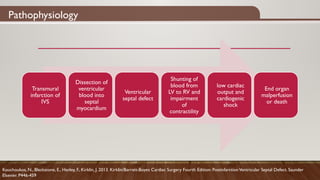
Pathophysiology
Transmural
infarction of
IVS
Dissection of
ventricular
bloodinto
septal
myocardium
Ventricular
septal defect
Shunting of
blood from
LV to RV and
impairment
of
contractility
low cardiac
output and
cardiogenic
shock
End organ
malperfusion
or death
Kouchoukos, N., Blackstone, E., Hanley, F., Kirklin, J. 2013. Kirklin/Barratt-Boyes Cardiac Surgery Fourth Edition: PostinfarctionVentricular Septal Defect. Saunder
Elsevier. P446-459
8.
Clinical Features
• Developmentof pansystolic murmur (lower sternal border) after recent MI (may be from acute
mitral regurgitation as well)
• CXR Pulmonary venous hypertension and increased pulmonary blood flow
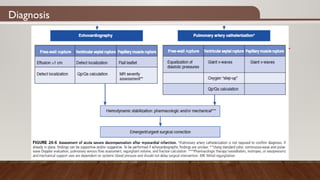
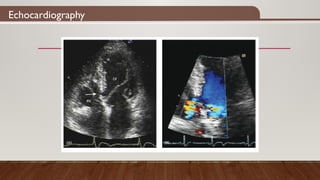
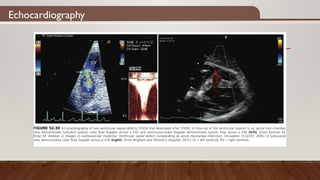
• TTE/TOE with Dopple color flow imaging to define the site of theVSD, quantify magnitude of
shunting, ascertain presence of mitral regurgitation
• Introduction of Swan-Ganz catheter obtain blood samples from cardiac chambers to quantify
Qp/Qs (usually 2.0 or greater). PAWP and PAP are usually elevated
• Coronary angiography in hemodynamically stable patients
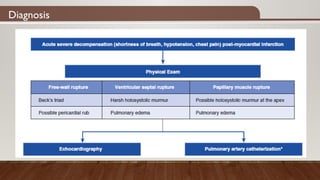
Diagnosis
• PostinfarctionVSD developedin 1%-3% of patients before the advent of thrombolytic
therapy and acute PCI.
• After these interventions, the frequency has been reduced to less than 0.5%.
• Without treatment, early death is common (<30% patients survive 2 weeks, only 10-20%
survive more than 4 weeks)
• Women and the elderly may be more susceptible
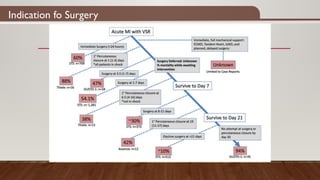
Indication fo Surgery
•PostinfarctionVSD is almost always and indication for operation
• The operation is usually done 2 to 3 weeks after the rupture so the edges of the defect have
become more fibrotic.The delay has to be with high certainty of hemodynamics stability.
• Criteria for deferment:
• Adequate cardiac output with no evidence of cardiogenic shock
• Absence of symptoms of pulmonary venous hypertension or easy control of initial symptoms with
appropriate drug therapy
• Absence of fluid retention
• Adequate renal function with stable BUN and creatinine levels
16.
Indication fo Surgery
•If the rupture leads to deteriorating hemodynamics with cardiogenic shocks, fluid retention and
pulmonary venous hypertension, deteriorating renal function immediate study and urgent
operation are indicated
• The risk of early repair is accepted because of the high risk of death without operation
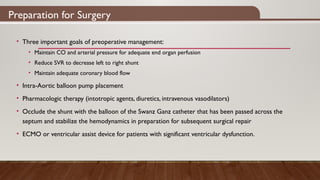
Preparation for Surgery
•Three important goals of preoperative management:
• Maintain CO and arterial pressure for adequate end organ perfusion
• Reduce SVR to decrease left to right shunt
• Maintain adequate coronary blood flow
• Intra-Aortic balloon pump placement
• Pharmacologic therapy (intotropic agents, diuretics, intravenous vasodilators)
• Occlude the shunt with the balloon of the Swanz Ganz catheter that has been passed across the
septum and stabilize the hemodynamics in preparation for subsequent surgical repair
• ECMO or ventricular assist device for patients with significant ventricular dysfunction.
19.
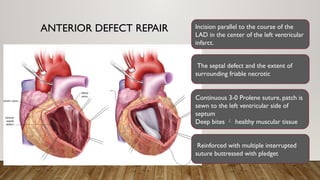
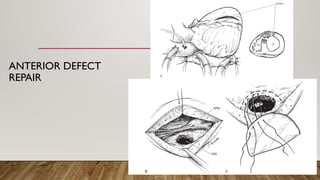
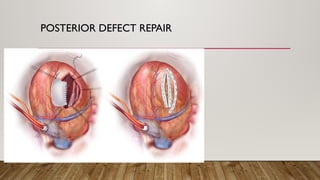
ANTERIOR DEFECT REPAIRIncision parallel to the course of the
LAD in the center of the left ventricular
infarct.
The septal defect and the extent of
surrounding friable necrotic
Continuous 3-0 Prolene suture, patch is
sewn to the left ventricular side of
septum
Deep bites healthy muscular tissue
Reinforced with multiple interrupted
suture buttressed with pledget
20.
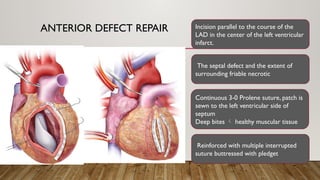
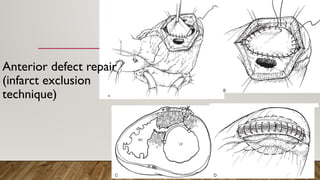
ANTERIOR DEFECT REPAIRIncision parallel to the course of the
LAD in the center of the left ventricular
infarct.
The septal defect and the extent of
surrounding friable necrotic
Continuous 3-0 Prolene suture, patch is
sewn to the left ventricular side of
septum
Deep bites healthy muscular tissue
Reinforced with multiple interrupted
suture buttressed with pledget
#2 The timing correlates with the maximal tissue necrosis from acute MI with minimal healing occurred.
Older age and total occlusion of the infarct vessel with minimal collateralization are associated with postinfarction VSD
The onset of early coronary perfusion using thrombolytics or angioplasty may have shortened the time between infarction and septal rupture due to hemorrhagic reperfusion
#19 Inotropic improve end organ perfusion in the face of impaired rv or lv function
Diuretics treat pulmonary edema
Vasodilators occasionally helpful, most patients are hypotensive