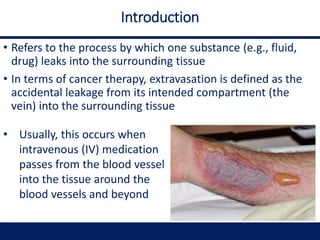
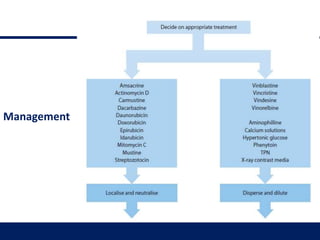
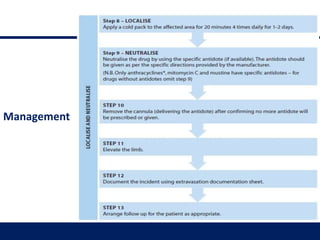
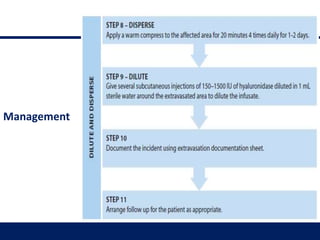
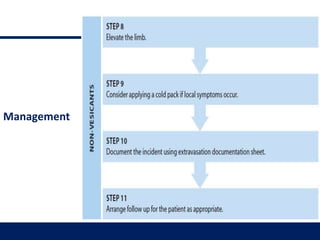
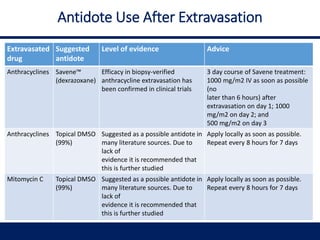
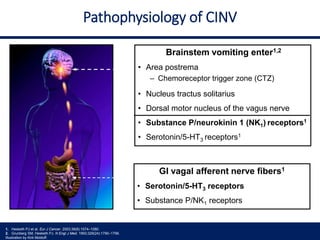
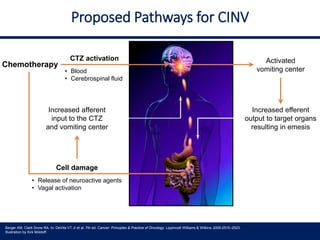
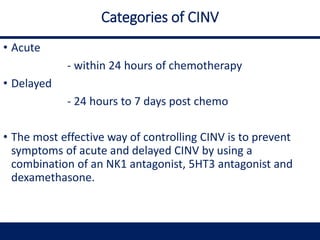
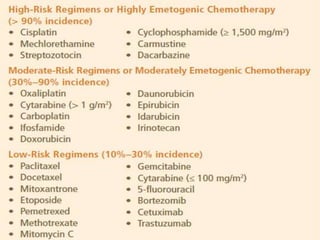
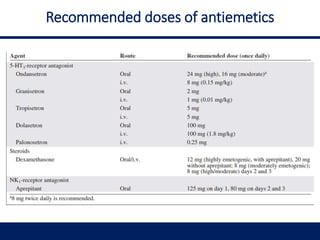
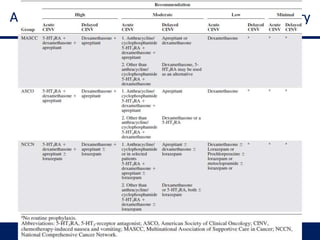
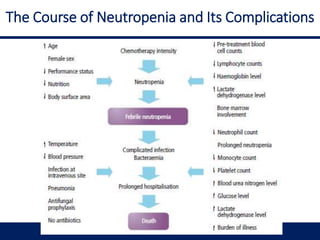
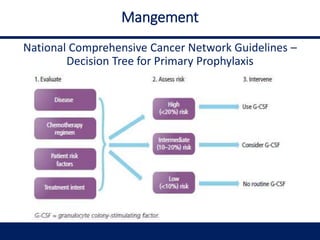
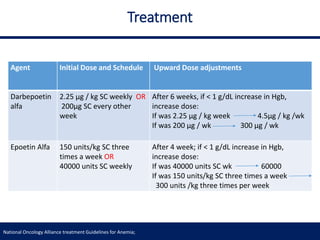
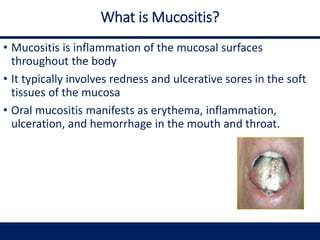
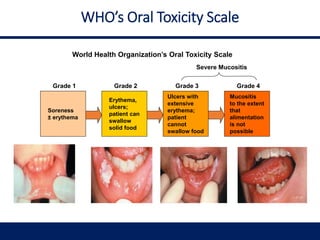
This document provides information on post-chemotherapy care and management of side effects. It discusses extravasation, which is when chemotherapy leaks from the vein into surrounding tissue. It classifies extravasation reactions and describes how to recognize and manage it. It also covers chemotherapy-induced nausea and vomiting (CINV), discussing pathophysiology and providing recommendations for preventing nausea based on emesis risk. The document further addresses febrile neutropenia, defining it and outlining management strategies. It then discusses anemia as a side effect of chemotherapy and radiation, describing treatment goals and options. Finally, the document defines mucositis as inflammation of mucosal surfaces throughout the body.

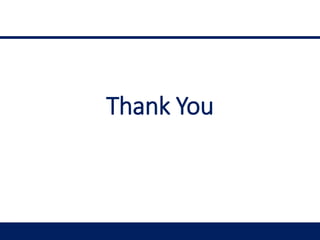
![Management of oral mucositis
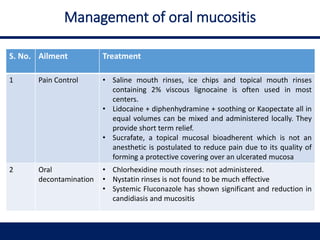
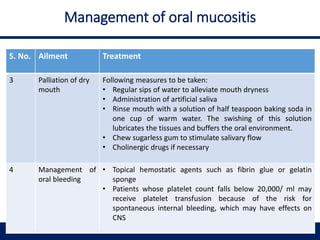
S. No. Ailment Treatment
5 Therapeutic
intervention for
oral mucositis
Cryotherapy
• Ice-chips are placed in the oral cavity, five minutes prior to
chemotherapy and replenished as needed for up to 30
minutes
• Cryotherapy is useful for short bolus chemotherapy
Growth factors
• Human keratinocyte growth factor -1 [paliferamin],
significantly reduces incidence of WHO grade 3 and 4 oral
mucositis
Anti-inflammatory agents
• Oral suspension of L-glutamine reduced the incidence of
clinically significant chemotherapy-induced oral mucositis
• Antioxidants
Antioxidants
• N-Acetylcysteine in a proprietary matrix for topical
application in the oral cavity](https://image.slidesharecdn.com/postchemotherapycarever1-200605115539/85/Post-chemotherapy-care-ver-1-0-44-320.jpg)









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
