• Over thelast decade, the Global Polio Eradication Initiative (GPEI)
made steady progress on the path to eradication.
• Wild poliovirus types 2 and 3 (WPV2 and WPV3) were declared
eradicated in 2015 and 2019, respectively;
• the World Health Organization (WHO) South-East Asia Region was
declared free of poliovirus in 2014; and
• most recently, the WHO African Region was certified free of wild
poliovirus (WPV) in August 2020.
4.
• In thefinal two endemic countries, Afghanistan and Pakistan, wild
poliovirus type 1 (WPV1) persists alongside circulating vaccine-
derived poliovirus type 2 (cVDPV2).
• Globally, cVDPV2 outbreaks have accelerated in countries that have
been free from WPV1, with outbreaks occurring in four of the six
geographical regions of WHO.4
5.
Strategy builds ontwo primary goals based on the current state of the
eradication effort:
Goal One to permanently interrupt all poliovirus transmission in
endemic countries and
Goal Two to stop cVDPV transmission and prevent outbreaks in non-
endemic countries.
6.
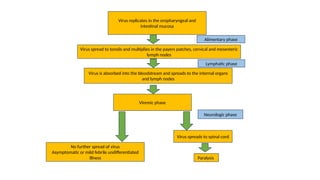
Paralysis
Virus spreads tospinal cord
Neurologic phase
No further spread of virus
Asymptomatic or mild febrile undifferentiated
illness
Viremic phase
Virus is absorbed into the bloodstream and spreads to the internal organs
and lymph nodes
Lymphatic phase
Alimentary phase
Virus spread to tonsils and multiplies in the payers patches, cervical and mesenteric
lymph nodes
Virus replicates in the oropharyngeal and
intestinal mucosa
8.
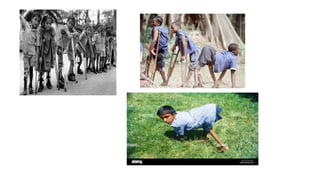
• Poliomyelitis isa crippling disease that results from infection with
any one of the three related poliovirus types (referred to as types
P1, P2, and P3), members of the enterovirus (picornavirus) family.
Poliovirus is transmitted from one person to another by oral
contact with secretions or faecal material from an infected
person. Once viral reproduction is established in the mucosal
surfaces of the nasopharynx, poliovirus can multiply in specialized
cells in the intestines and enter the blood stream to invade the
central nervous system, where it spreads along nerve fibres.
When it multiplies in the nervous system, the virus can destroy
nerve cells (motor neurons) which activate skeletal muscles.
9.
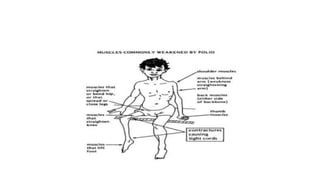
• These nervecells cannot regenerate, and the affected muscles
lose their function due to a lack of nervous enervation - a
condition known as acute flaccid paralysis (AFP). Typically, in
patients with poliomyelitis muscles of the legs are affected more
often than the arm muscles. More extensive paralysis, involving
the trunk and muscles of the thorax and abdomen, can result in
quadriplegia. In the most severe cases (bulbar polio), poliovirus
attacks the motor neurons of the brain stem - reducing breathing
capacity and causing difficulty in swallowing and speaking.
Without respiratory support, bulbar polio can result in death. It
can strike at any age, but affects mainly children under three
(over 50% of all cases).
10.
• Acute FlaccidParalysis (AFP) Surveillance
• Nationwide AFP (acute flaccid paralysis) surveillance is the
gold standard for detecting cases of poliomyelitis. The four
steps of surveillance are:
1.finding and reporting children with acute flaccid paralysis
(AFP)
2.transporting stool samples for analysis
3.isolating and identifying poliovirus in the laboratory
4.mapping the virus to determine the origin of the virus
strain.
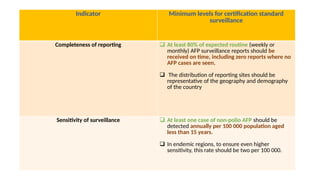
Indicator Minimum levelsfor certification standard
surveillance
Completeness of reporting At least 80% of expected routine (weekly or
monthly) AFP surveillance reports should be
received on time, including zero reports where no
AFP cases are seen.
The distribution of reporting sites should be
representative of the geography and demography
of the country
Sensitivity of surveillance At least one case of non-polio AFP should be
detected annually per 100 000 population aged
less than 15 years.
In endemic regions, to ensure even higher
sensitivity, this rate should be two per 100 000.
13.
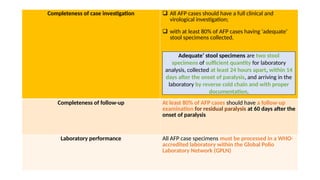
Completeness of caseinvestigation All AFP cases should have a full clinical and
virological investigation;
with at least 80% of AFP cases having ‘adequate’
stool specimens collected.
Completeness of follow-up At least 80% of AFP cases should have a follow-up
examination for residual paralysis at 60 days after the
onset of paralysis
Laboratory performance All AFP case specimens must be processed in a WHO-
accredited laboratory within the Global Polio
Laboratory Network (GPLN)
Adequate’ stool specimens are two stool
specimens of sufficient quantity for laboratory
analysis, collected at least 24 hours apart, within 14
days after the onset of paralysis, and arriving in the
laboratory by reverse cold chain and with proper
documentation.
14.
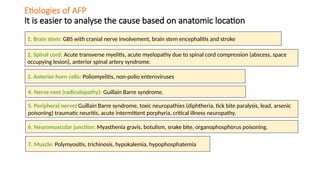
Etiologies of AFP
Itis easier to analyse the cause based on anatomic location
2. Spinal cord: Acute transverse myelitis, acute myelopathy due to spinal cord compression (abscess, space
occupying lesion), anterior spinal artery syndrome.
3. Anterior horn cells: Poliomyelitis, non-polio enteroviruses.
4. Nerve root (radiculopathy): Guillain Barre syndrome.
5. Peripheral nerve: Guillain Barre syndrome, toxic neuropathies (diphtheria, tick bite paralysis, lead, arsenic
poisoning) traumatic neuritis, acute intermittent porphyria, critical illness neuropathy.
7. Muscle: Polymyositis, trichinosis, hypokalemia, hypophosphatemia.
6. Neuromuscular junction: Myasthenia gravis, botulism, snake bite, organophosphorus poisoning.
1. Brain stem: GBS with cranial nerve involvement, brain stem encephalitis and stroke
15.
Polio can beeradicated because of the following characteristics:
• poliovirus has no animal reservoir;
• poliovirus survives for a limited amount of time in the environment;
and
• inexpensive and effective vaccines exist to protect the population
from the disease.
Editor's Notes
#5 Achieving eradication through collective ownership and accountability The Polio Eradication Strategy 2022–2026 offers a comprehensive set of actions to strengthen the GPEI so it is fit for purpose. To be successful, the programme must operate with an emergency tempo while it also becomes more accountable to the collective partnership, more responsive to the intersecting needs of impacted communities, more welcoming of sociological, anthropological and health economic expertise, and more integrated with social and health programmes that deliver critical interventions to vulnerable populations. These actions, many of which are underway in 2021, will empower the GPEI to meet challenges head-on and achieve and sustain a polio-free world.
To achieve these goals, the GPEI will transform its approach in each region and country through five mutually reinforcing objectives.



































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















