LECTURE OUTLINE
1. Introduction
2.Definition
3. Epidemiology
4. Risk factors
5. Classification
6. Etiology
7. Pathogenesis
8. History and Clinical features
9. Investigations
10. Complications
11. Management
12. Prevention
3.
INTRODUCTION
Globally, pneumonia isa significant cause of morbidity and
mortality in children younger than 5 years throughout the world,
particularly in developing countries.
The introduction of immunisation ( Hib and Pneumococcal) has
drastically reduced the incidence and mortality due to
pneumonia.
4.
DEFINITION
Pneumonia is aninflammation of the parenchyma of
the lungs.
Most cases of pneumonia are caused by
microorganisms, but there are several noninfectious
causes
5.
EPIDEMIOLOGY
An estimated 120million cases of pneumonia occur annually
worldwide, resulting in1.3 millions deaths.
Children below the age of 2 years in the developing world, account
for nearly 80% of Paediatric deaths secondary to pneumonia.
The introduction of vaccines ( Hib and pneumococcal) has to a
certain degree reduced the risk of pneumonia in developing
countries
ETIOLOGY
Causes of pneumoniain children can be classified by age-specific versus
pathogen-specific organisms
1. Neonates:
Early-Onset: 2-5 years
• Group B streptococci . Streptococcus pneumoniae
• Klebsiella pneumoniae . Hemophilus influenzae
• Escherichia coli . Respiratory viruses
• Listeria monocytogenes
Late onset: 5 years and above
• Streptococcus pneumoniae . S. pneumoniae
• Streptococcus pyogenes . Mycoplasma pneumoniae
• Staphylococcus aureus
S. Pneumoniae is still the most commonly identified organism in children of 5 years and above.
10.
Congenital infections
TORCHinfections can potentially cause pneumonia
in newborn babies
Toxoplasmosis
Others –HIV
Rubella
CMV
Herpes simplex
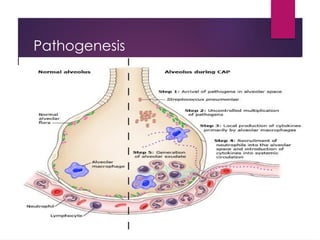
PATHOGENESIS
Pneumonia is dueto an invasion of the lower respiratory tract, below the larynx
by pathogens either by inhalation, aspiration, respiratory epithelium invasion or
hematogenous spread.
The infection breaches the anatomical barriers, humoral and cellular immunity
either by fomite/droplet spread ( mostly viral) or nasopharyngeal colonisation
( mostly bacterial). This leads to inflammation causing an exudative process,
which in turns impairs oxygenation.
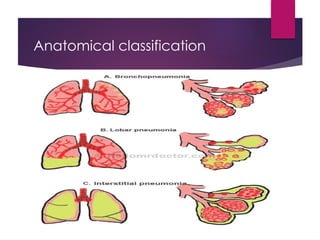
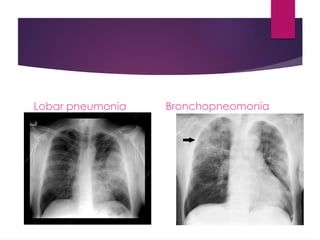
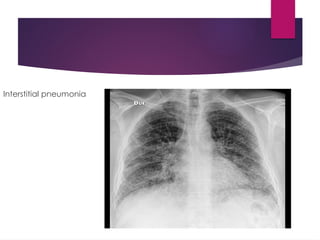
There are 4 stages of lobar pneumonia:
1. Alveolar oedema and vascular congestion: within 24 hours
2. Red hepatisation: consolidation due to RBCs, neutrophils and
desquamated epithelial cells associated with fibrin deposits in the alveoli
3. Gray hepatisation: 2 -3 days later. Lung appear dark brown. There
accumulation of hemosiderin and hemolysis of RBCs
4. Resolution: cellular infiltrate is resorbed and the pulmonary architecture is
HISTORY
Duration ofsymptoms
Exposures, travel,
Sick contacts
Baseline health of the child
Chronic diseases
Recurrent symptoms
Immunisation history
Maternal health
Birth complications in neonates.
18.
CLINICAL FEATURES
1. Symptoms:
Cough
Body hotness
Fast and difficult breathing
Feeding difficulty in infants
2. Signs:
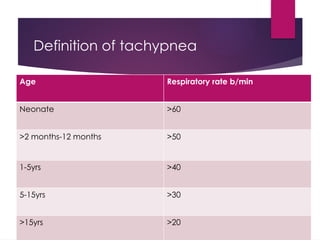
Tachypnoea
Inter and sub-costal recessions
Nasal flaring
Cyanosis
Sa O2 < 90% on room air
19.
PHYSICAL EXAMINATION
Inspection
• ill-looking
•chills/rigors
• Inter and sub-costal recessions
• Nasal flaring
• cyanosis
Palpation
• decreased chest expansion or
asymetry
• lymphadenopathy
• increased tactile fremitus
creaPercussion
• dull
• Stony dull, Hyperresonant
Auscultation
• bronchial breath sounds in periphery
• decreased air entry, crepitations
( coarse crackles )
• bronchophony -voice heard
abnormally clearly over consolidated
lung
• egaphony - listen to patient's chest as
they make "e" sound, if +'ve will hear
an "a" sound
• whispering pectoriloquay - pt
whispers "1, 2, 3, 4", if clear then
extreme consolidation
INVESTIGATIONS
1. FBC +Acute phase reactants ( ESR and CRP)
2. CXR
3. Blood culture
4. Serology is being used to determine the presence
of mycoplasma, legionella, and chlamydia
species.
5. Sputum mcs
CLINICAL Classification
Pneumonia-cough fever breathing difficulties
Severe Pneumonia- fever, cough, breathing
difficulties, crepitations
Very severe Pneumonia- above symptoms PLUS
cyanosis, head bobbing, inability to take orally
25.
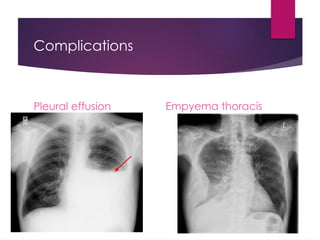
COMPLICATIONS
Local
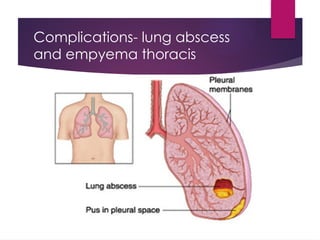
1. Empyema: acollection of pus in
the pleural cavity
2. Pleural effusion: build-up of
excess fluid between the layers
of the pleura outside the lungs
3. Lung abscess
4. Necrotizing pneumonia*
5. Respiratory failure
Systemic
Sepsis
SiADH
Hypoxic injury to vital organs-
Brain,heart,kidneys
TREATMENT
Treatment should betargeted to a specific pathogen
that is suspected based on information obtained from
history and physical exam.
1. Supportive and symptomatic management is key
and includes supplemental oxygen for hypoxia,
antipyretics for fever, and fluids for dehydration.
2. Specific antibiotics
3. Promote good nutrition + breastfeeding
4. Treat complications-
29.
Viral pneumonias
Virusesthat can lead to pneumonia include:
Influenza (flu) A and B viruses, the most common causes in adults
Respiratory syncytial virus (RSV), which is more common in infants and
children than in adults
Coronaviruses, including SARS-CoV-2, the new virus that causes
COVID-19
Rhinoviruses, parainfluenza viruses, and adenoviruses
30.
Symptoms
Similar tobacterial pneumonia except:
Dry cough
Low grade fever
Running nose
myalgia
31.
Treatment
A-clear airway,B-oxygen, C-IV access
Supportive –
Analgesia, antipyretic, NS nasal drops
Hydration
If you have an influenza virus, medications such as oseltamivir (Tamiflu),
zanamivir (Relenza), or peramivir (Rapivab). These drugs keep flu viruses
from spreading in your body.
If RSV is the cause of your pneumonia, a medication such as ribavirin (
Virazole) may be given, especially vulnerable patients with CHD,
immunocpmromisation. This helps to limit the spread of viruses.
32.
Clinical setting-HAP/VAP
Hospital-acquiredpneumonia (HAP) or nosocomial pneumonia refers
to any pneumonia contracted by a patient in a hospital at least 48–
72 hours after being admitted.
It is thus distinguished from community-acquired pneumonia.
It is usually caused by a bacterial infection, rather than a virus.
33.
HAP
Accounts for15–20% of the total.
It is the most common cause of death among nosocomial infections
and is the primary cause of death in intensive care units
HAP typically lengthens a hospital stay by 1–2 weeks.
34.
Causes of HAP
The majority of cases, rod shaped gram-negative organisms (52%)
Staphylococcus aureus (19%), usually of the MRSA type.
Others are Haemophilus spp. (5%).
In the ICU results were S. aureus (17.4%), Pseudomonas aeruginosa
(17.4%), Klebsiella pneumoniae and Enterobacter spp. (18.1%), and
Haemophilus influenzae (4.9%).
Viral pneumonia: influenza and respiratory syncytial virus and, in the
immunocompromised host, cytomegalovirus – cause 10–20% of
infections.[2]
35.
Clinical features ofHAP
New or progressive infiltrate on the chest X-ray with one of the
following:[3]
Fever > 37.8 °C (100 °F)
Purulent sputum
Leukocytosis > 10,000 cells/μl
36.
Risk factors forHAP
Among the factors contributing to contracting HAP are
mechanical ventilation (ventilator-associated pneumonia)
Old age,
Decreased filtration of inspired air, intrinsic respiratory, neurologic, or
other disease states that result in respiratory tract obstruction,
Trauma, (abdominal) surgery, medications, or decreased clearance
of secretions may diminish the defenses of the lung.
Also, poor hand-washing and inadequate disinfection of respiratory
devices cause cross-infection and are important factors.
37.
VAP
Ventilator-associated pneumonia(VAP) is a sub-type of hospital-acquired
pneumonia (HAP) which occurs in people who are receiving mechanical
ventilation.
A positive culture after intubation is indicative of ventilator-associated
pneumonia and is diagnosed as such.
In order to appropriately categorize the causative agent or mechanism it is
usually recommended to obtain a culture prior to initiating mechanical
ventilation as a reference.
Treatment
A-clear airway,B-oxygen, C-IV access D- check RBS
Usually, initial therapy is empirical.
Then titrated to culture specific antibiotics
Supportive- Antipyretic/analgesis, feeds, fluids,
Treat complications e.g,drain empyema thoracis, thoracocentesis for
symptomatic effusions
40.
PREVENTION
1. Avoid overcrowding
2.Immunisation:
Pneumococcal conjugate (PCV)
Haemophilus influenzae type b (Hib)
Pertussis (whooping cough)
Measles
3. Observe general hygiene, hand hygiene by HCW to
prevent cross infection
4. Breastfeeding during the first 6 months of life
5. Promote good nutrition
#12 If the healing is not ideal, then then it may lead to parapneumonic effusions and pleural adhesions.
#25 *In children, necrotizing pneumonia (NP) is an uncommon, severe complication of pneumonia. It is characterized by destruction of the underlying lung parenchyma resulting in multiple small, thin-walled cavities and is often accompanied by empyema and bronchopleural fistulae

![Causes of HAP
The majority of cases, rod shaped gram-negative organisms (52%)
Staphylococcus aureus (19%), usually of the MRSA type.
Others are Haemophilus spp. (5%).
In the ICU results were S. aureus (17.4%), Pseudomonas aeruginosa
(17.4%), Klebsiella pneumoniae and Enterobacter spp. (18.1%), and
Haemophilus influenzae (4.9%).
Viral pneumonia: influenza and respiratory syncytial virus and, in the
immunocompromised host, cytomegalovirus – cause 10–20% of
infections.[2]](https://image.slidesharecdn.com/pneumoniainchildren-250413170550-5b5d1c6f/85/PNEUMONIA-IN-CHILDREN-PRESENTATION-MADE-SIMPLE-34-320.jpg)
![Clinical features of HAP
New or progressive infiltrate on the chest X-ray with one of the
following:[3]
Fever > 37.8 °C (100 °F)
Purulent sputum
Leukocytosis > 10,000 cells/μl](https://image.slidesharecdn.com/pneumoniainchildren-250413170550-5b5d1c6f/85/PNEUMONIA-IN-CHILDREN-PRESENTATION-MADE-SIMPLE-35-320.jpg)