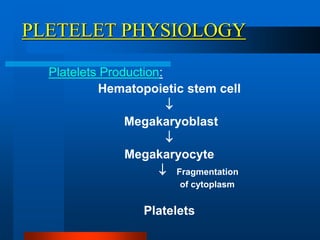
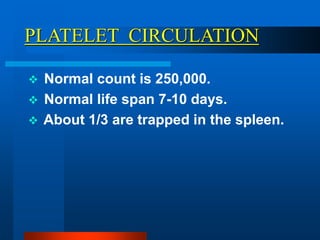
Platelets are produced from megakaryocytes in the bone marrow and normally circulate in the bloodstream for 7-10 days. They play a key role in hemostasis through adhesion, secretion of factors, and aggregation at sites of vascular injury. Thrombocytopenia refers to a low platelet count and can result from decreased production or increased destruction. Immunothrombocytopenia is an autoimmune disorder where antibodies destroy platelets. Defects in platelet function despite normal counts can also cause bleeding disorders.

































































![[Esthiningrum Dewi Agustin_JR_290125].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/esthiningrumdewiagustinjr290125-250305000543-5c8a7bdd-thumbnail.jpg?width=640&height=640&fit=bounds)





















