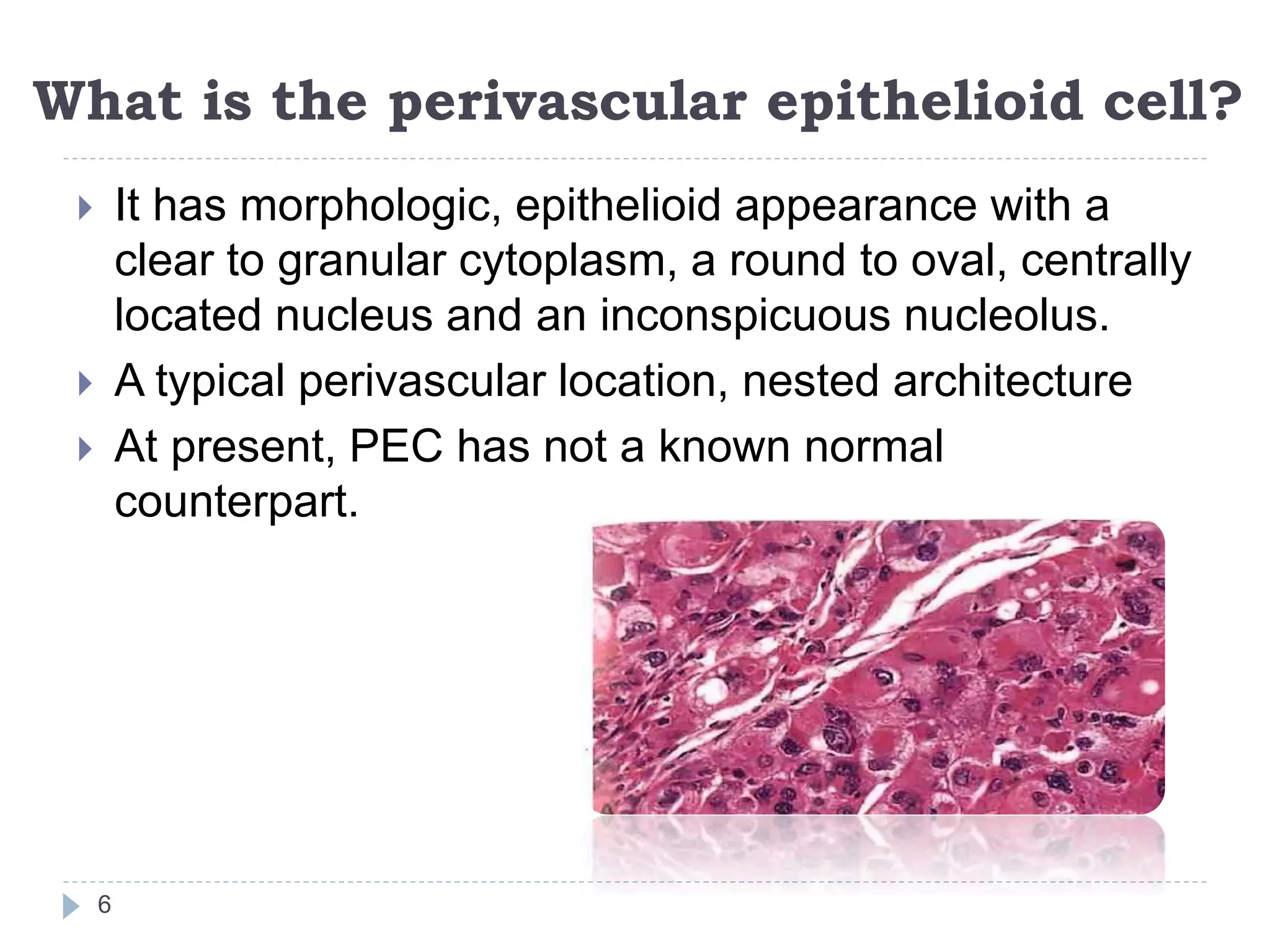
Perivascular epithelioid cell tumors (PEComas) are mesenchymal neoplasms defined by the presence of distinctive perivascular epithelioid cells. They can arise in various organs. Angiomyolipoma and lymphangioleiomyomatosis are examples of PEComas that arise in the kidney and lung respectively. Angiomyolipoma is a typically benign tumor composed of blood vessels, smooth muscle, and fat cells, while lymphangioleiomyomatosis involves proliferation of perivascular epithelioid cells around lymphatics leading to cyst formation in the lungs. The pathological features, diagnosis, and management of these PEComa subtypes were discussed in