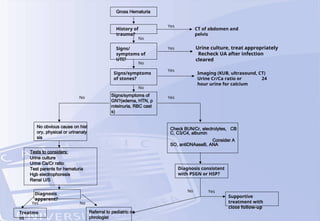
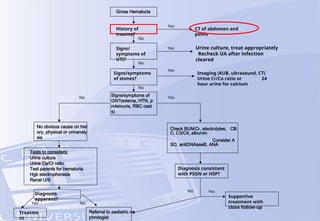
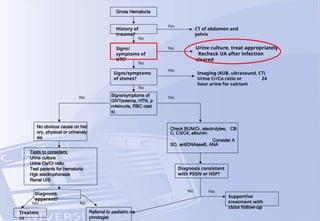
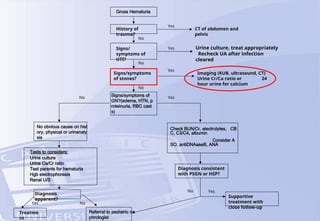
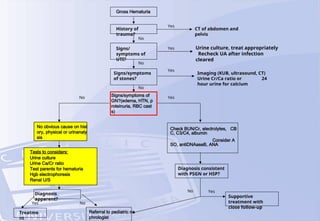
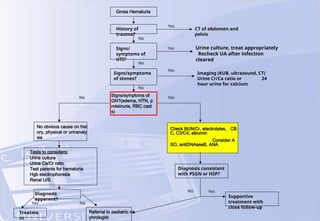
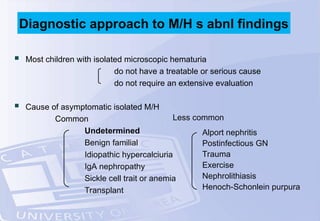
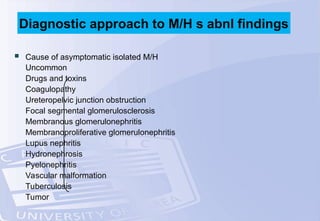
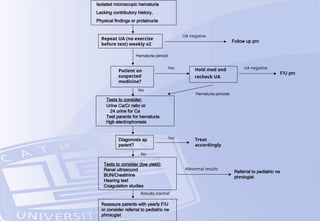
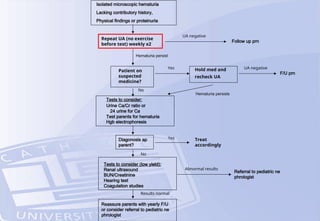
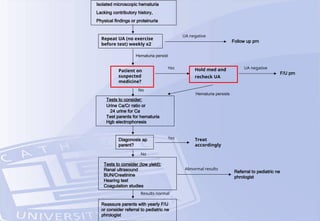
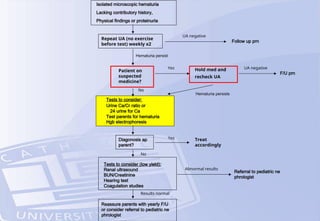
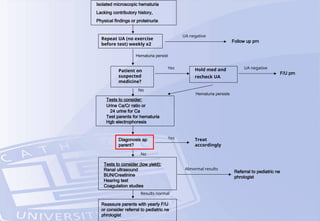
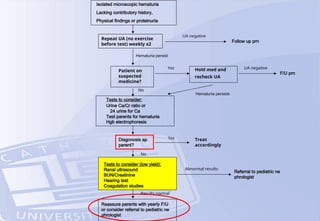
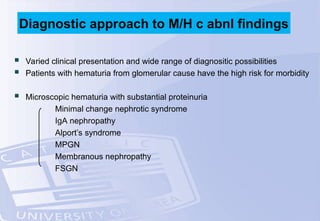
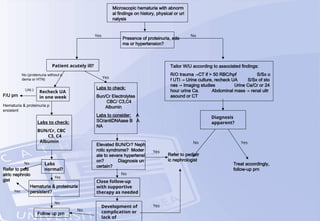
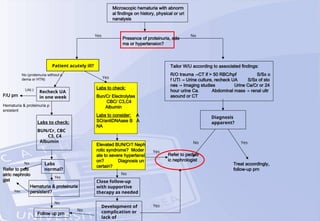
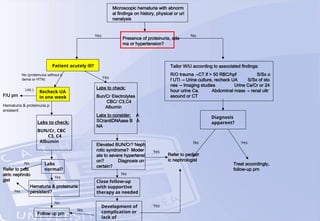
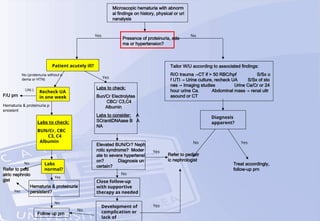
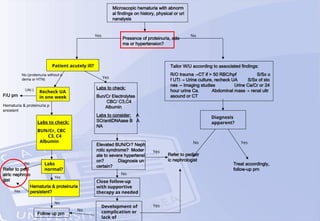
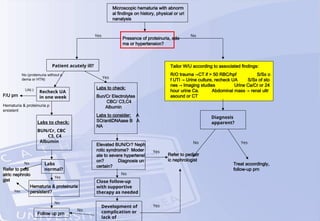
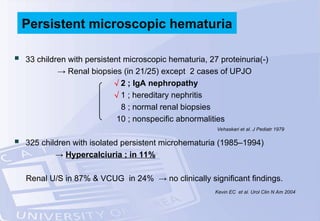
The document discusses the evaluation of hematuria in children, emphasizing its significance as a marker for renal or bladder diseases, while differentiating between gross and microscopic hematuria. It outlines a systematic approach for assessment, including initial history and physical examinations, laboratory tests, and recommendations for further evaluation based on findings. It acknowledges that most children with isolated microscopic hematuria do not require extensive evaluation unless there are concerning symptoms or abnormal findings.





















































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)



![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)










