Contents
1. Is ithaematuria?What else could it be?
2. Microscopic vs macroscopic
3. Urological vs Nephrological?
4. History and exam
5. Microscopy
6. Investigations
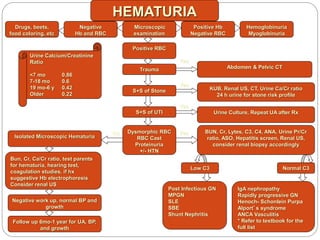
7. Algorithm!
3.
Vignette No. 1
12 year old girl presents with abdominal pain and
macroscopic haematuria for past 24 hours, 2 vomits
She has had low grade fever and coryzal symptoms as well
What else would you like to ask on history?
Does the fact she has pain change your mind?What about the
viral symptoms?
Her BP is 125/78, HR 90, afebrile, JVP 5cm, parents think
she may have periorbital swelling. Mild pedal edema.The
urine in the jar next to the bed is a reddy-brown colour.
Urinalysis: SG 1015 blood ++++ protein +++
What is likely going on here?
You may now order tests!What would you like?
4.
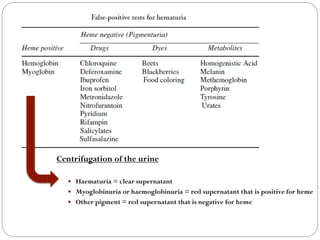
Urine colors?
Redto brown – hematuria, hemoglobinuria, myoglobinuria
White—phosphaturia, pyuria, chyluria
Brown black—alkaptonuria (on prolonged standing), methemoglobin,
myoglobin
Green—triamterene, amitriptyline, propofol, and pseudomonas
infection
Blue—methylene blue
Brown urine—chloroquine, nitrofurantoin
Darkening on standing—imipenem, methyldopa, metronidazole
Pink urine—uric acid crystalluria
Orange—rifampicin, warfarin
Cloudy—usually due to crystal formation on standing, uric acid crystals
form in acidic urine, phosphate crystals form in alkaline urine
5.
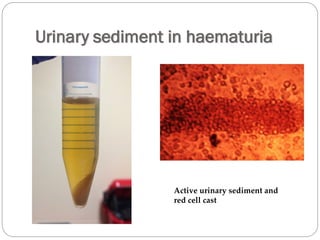
Centrifugation of theurine
Haematuria = clear supernatant
Myoglobinuria or haemoglobinuria = red supernatant that is positive for heme
Other pigment = red supernatant that is negative for heme
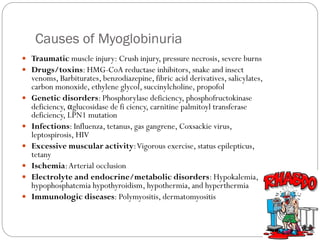
Causes of Myoglobinuria
Traumatic muscle injury: Crush injury, pressure necrosis, severe burns
Drugs/toxins: HMG-CoA reductase inhibitors, snake and insect
venoms, Barbiturates, benzodiazepine, fibric acid derivatives, salicylates,
carbon monoxide, ethylene glycol, succinylcholine, propofol
Genetic disorders: Phosphorylase deficiency, phosphofructokinase
deficiency, αglucosidase de fi ciency, carnitine palmitoyl transferase
deficiency, LPN1 mutation
Infections: Influenza, tetanus, gas gangrene, Coxsackie virus,
leptospirosis, HIV
Excessive muscular activity:Vigorous exercise, status epilepticus,
tetany
Ischemia:Arterial occlusion
Electrolyte and endocrine/metabolic disorders: Hypokalemia,
hypophosphatemia hypothyroidism, hypothermia, and hyperthermia
Immunologic diseases: Polymyositis, dermatomyositis
8.
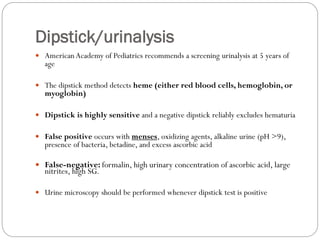
Dipstick/urinalysis
American Academyof Pediatrics recommends a screening urinalysis at 5 years of
age
The dipstick method detects heme (either red blood cells, hemoglobin, or
myoglobin)
Dipstick is highly sensitive and a negative dipstick reliably excludes hematuria
False positive occurs with menses, oxidizing agents, alkaline urine (pH >9),
presence of bacteria, betadine, and excess ascorbic acid
False-negative: formalin, high urinary concentration of ascorbic acid, large
nitrites, high SG.
Urine microscopy should be performed whenever dipstick test is positive
9.
Microscopic Hematuria
Microscopichematuria is common in children
Usually an incidental finding on urinalysis
> 5 RBC per high power field (HPF) on fresh, centrifuged sample
In one study
3 - 4 % of unselected school-age children between 6 to 15 years of age had a
positive dipstick for blood in a single urine sample.
This falls to 1 percent or less for two or more positive samples.
Among the 1 percent of children with two or more positive urines for
hematuria, only one-third have persistent hematuria, defined as a positive
repeat test after six months.
10.
Microscopic Hematuria
Ina study of 342 children with asymptomatic
microscopic hematuria, evaluation included
o Complete blood count
o Urinalysis
o Serum creatinine
o C3
o Ultrasonography or intravenous pyelography
Results
o No diagnosis was made in 80 %
o The most common was hypercalciuria
• 16 %-30%
11.
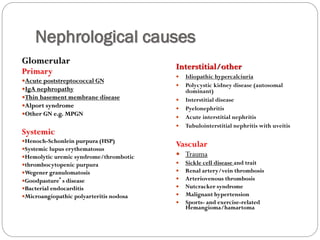
Causes of microhaematuria
Isolated and intermittent: not of concern
The most common causes of PERSISTENT microscopic
hematuria include:
Glomerulopathies
o IgA nephropathy
o Alport syndrome
o Thin basement membrane disease (TBMD)
o Postinfectious glomerulonephritis
Hypercalciuria
12.
Macroscopic Haematuria
Definition:visible to the naked eye
Gross hematuria in children is relatively unusual
1 in 1000 outpatient visits to a pediatrician.
Color change does not reflect degree of blood loss
1 mL of blood per liter of urine is visible
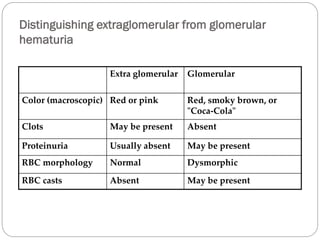
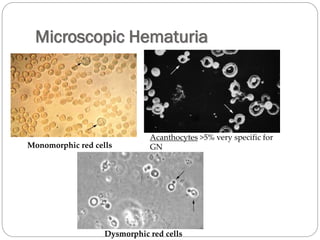
Distinguishing extraglomerular fromglomerular
hematuria
Extra glomerular Glomerular
Color (macroscopic) Red or pink Red, smoky brown, or
"Coca-Cola"
Clots May be present Absent
Proteinuria Usually absent May be present
RBC morphology Normal Dysmorphic
RBC casts Absent May be present
16.
Vignette 2
6year old boy is seen in Emergency for a chest infection.
They dipstick his urine.You are the Registrar so they call you
over:
There is microscopic haematuria
What else would you want to know?
Turns out it is isolated microscopic haematuria
You are now the clinic person!You see him again at 3 and 6
months. Each time he has persistent microscopic haematuria
with no other abnormalities.
What if there were some urine samples in between with no
blood at all?
17.
History
The descriptionof the urine should be specific
Urine in glomerular disease
uniformly discolored, without clots, dark brown, like tea or
coca-cola.
Urine in lower urinary tract or vascular bleeding
bright red or cherry-colored
yellow but blood unevenly mixed with the urine or with blood
clots
urinary bleeding that only appears at the initiation of a void or
at the end of a void (terminal)
18.
History
Pain
Thecharacter may be very informative
Lower urinary tract symptoms such as dysuria, urgency, and frequency imply
a urethritis or cystitis
History of unilateral flank pain that may radiate to the groin +/- vomiting
suggests obstruction caused by a calculus or blood clot
Gross hematuria from parenchymal disease may occasionally be accompanied
by dull loin or abdominal pain e.g. pyelonephritis, PSGN, HSP due to stretch
on renal capsule
Recurrent, painless gross hematuria is often seen in young patients with IgA,
MPGN orTBMD
Bleeding from Urological causes (tumours, cyst accident, UPJ) can occur
spontaneously or after minor trauma with accompanying pain - check for a
mass
19.
History
History ofinfection, fever
Recent pharyngitis, skin infection, or other febrile illnesses
Systemic manifestations
Shortness of breath, edema, or weight gain from fluid retention.
Arthralgias, arthritis, weight loss, Ulcers, Hemoptysis, rash, etc.
Bleeding disorder
Sickle cell
Other bleeding, such heavy menses, prolonged nosebleeds, and
bleeding associated with surgical procedures
Activities
Extreme exercise, such as marathon running
Medication history
NSAID, Cyclophosphamide
Family history
End-stage renal failure/Transplant
Stones
Deafness or Alport syndrome
Cystic diseases
20.
Physical Examination
Fever
JVP and Blood pressure
Weight gain
Growth
Edema
Pallor
Respiratory distress
Skin rashes
Abdominal or flank masses
Genitalia
Musculoskeletal
Gross appearance of urine (see yourself)
DIPSTICK
21.
Vignette No. 3
16 yr old male presents to ER with intermittent flank pain,
macrohaematuria, proteinuria ++
A number of episodes, off school, occasional vomit here and there
Questions?
What investigations?
They are all normal in between episodes
He returns and discloses a postural element to the pain
On examination, nothing to find except a left varicoele
You order an MRV looking for..
Nutcracker syndrome (or left renal vein entrapment
syndrome)
Laboratory Evaluations
…dependson the history, exam, urinalysis and
microscopy!
Reasonable to start with:
1. Urine microscopy, culture +/-viruses
2. Urine Ca2+:creatinine ratio
3. Urine protein:creatinine ratio (early morning sample)
4. Ultrasound kidneys and bladder +/- doppler
5. Consider: testing urea and creatinine, CBC,
glomerulonephritis screen including ASOT and C3,
and urinalysis of parents/siblings, sickle screen
26.
HEMATURIA
Drugs, beets,
food coloring,etc
Bun, Cr, Ca/Cr ratio, test parents
for hematuria, hearing test,
coagulation studies, if hx
suggestive Hb electrophoresis
Consider renal US
KUB, Renal US, CT, Urine Ca/Cr ratio
24 h urine for stone risk profile
Abdomen & Pelvic CT
Negative
Hb and RBC
Hemoglobinuria
Myoglobinuria
Positive Hb
Negative RBC
Microscopic
examination
Positive RBC
IgA nephropathy
Rapidly progressive GN
Henoch- Schonlein Purpa
Alport’s syndrome
ANCA Vasculitis
* Refer to textbook for the
full list
S+S of Stone
Trauma
Urine Calcium/Creatinine
Ratio
<7 mo 0.86
7-18 mo 0.6
19 mo-6 y 0.42
Older 0.22
S+S of UTI
Dysmorphic RBC
RBC Cast
Proteinuria
+/- HTN
Urine Culture, Repeat UA after Rx
Post Infectious GN
MPGN
SLE
SBE
Shunt Nephritis
Low C3
BUN, Cr, Lytes, C3, C4, ANA, Urine Pr/Cr
ratio, ASO, Hepatitis screen, Renal US,
consider renal biopsy accordingly
Isolated Microscopic Hematuria
Negative work up, normal BP and
growth
Follow up 6mo-1 year for UA, BP,
and growth
Normal C3
Yes
Yes
No
Yes
Yes