Downloaded 74 times

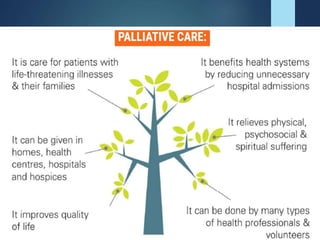



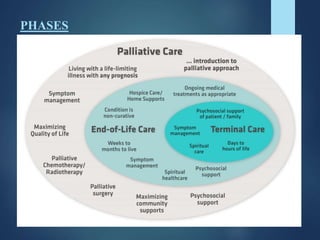



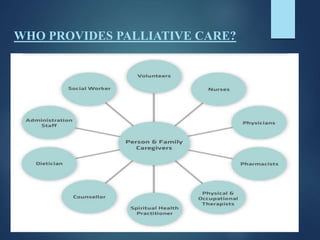
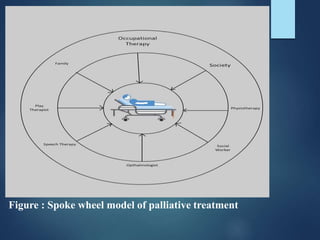
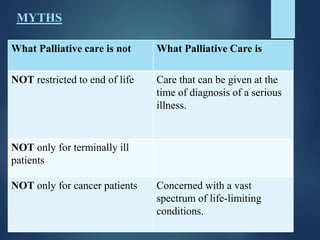
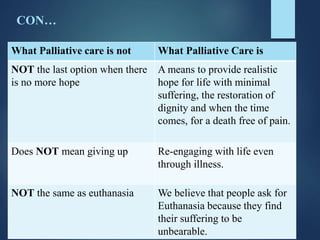
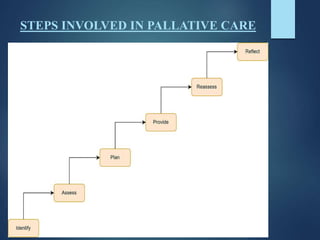
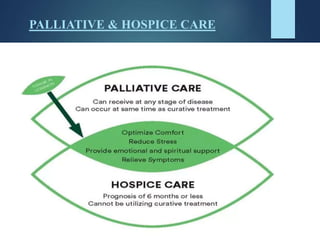
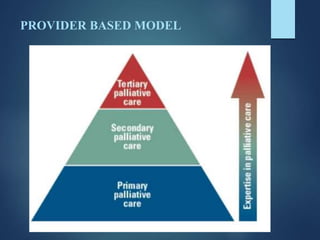

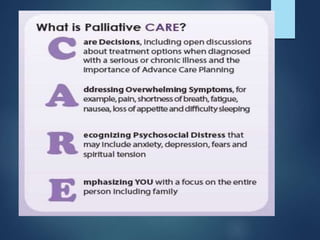



This document provides an overview of palliative care, including its definition, goals, scope, principles, and models. Palliative care aims to relieve suffering and improve quality of life for patients facing serious illnesses. It focuses on addressing physical, psychological, social, and spiritual needs through a holistic, team-based approach. While still limited in availability worldwide, palliative care services are expanding, especially to address needs for chronic disease management in addition to cancer care.



















































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)















