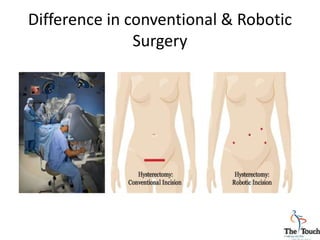
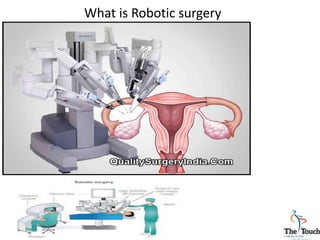
Robotic surgery has advantages over conventional and laparoscopic surgery for gynecological procedures. The da Vinci surgical system allows for precision in complex surgeries through its three-dimensional view and wristed instruments. Robotic surgery results in less blood loss, quicker recovery times, and fewer complications compared to open surgeries. While further research is still needed, robotic surgery has become a common method for hysterectomies and myomectomies to treat conditions like fibroids and cancer. The case study describes a large fibroid removed robotically with minimal blood loss and fast recovery for the patient.