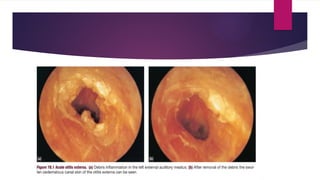
Otitis externa is a skin condition of the external auditory canal characterized by edema, erythema, and potential ear discharge, with various infectious and reactive causes. It can progress through inflammatory stages and is diagnosed based on clinical symptoms including pain and itching. Treatment involves regular ear cleaning, topical medications, and preventive measures to avoid recurrence.