This document provides an overview of Florence Nightingale's environmental theory of nursing. Some key points:
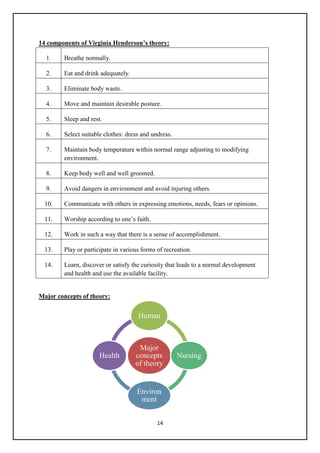
1) Nightingale established modern nursing and was the founder of nursing theory. She emphasized the importance of the patient's environment and proposed specific factors like ventilation, light, noise, and cleanliness that influence health.
2) Her theory defined nursing as putting the patient in the best condition for nature to act and separating it from medicine. She saw the environment as something that could be altered to promote patient health and healing.
3) Nightingale's theory focused on physical health factors but less on psychological needs. Nonetheless, her ideas revolutionized nursing and established it as a profession focused on environmental adaptations to






















![40
region. Her pattern is decided by others in the hospital. She
said, ―I am not able to mix up with others due to my
condition, I feel lonely.‖ Mrs Geetha‘s son stated, ―She is
very religious and bold enough to face the problems of life,
but now she has lost the confidence. She feels lonely and
isolated.‖ Mrs Geetha strives hard to achieve the fullest
health within her limits
related to activity intolerance
and inability to travel to usual
social activities.
4) Interrupted family process
related to financial crisis.
5) Anxiety related to prognosis
of the disease.
6) Risk for care giver strain
related to the chronic illness.
7) Knowledge deficit of the
caregiver related to homecare
management.
8) Risk for complications
related to the chronic illness.
Resonancy
Mrs Geetha is on treatment. She complies with it. She
states, ―If I do not take these medicines my condition may
deteriorate further.‖ She further states, ―My illness has laid
burden on my son.‖ But her son is very supportive. It is
observed that sometimes she is pleasant, sometimes dull
and withdrawn. When she was dull she said, ―I feel
depressed and guilty of my illness. I do not know what will
happen in the future?‖
Helicy
In Mrs Geetha‘s present condition she is unidirectional in
moving towards achieving health within her limits. She
said, ―I accept my illness; I may be recovering by using all
the resources available. I do not fear death.‖ Her son stated,
―We will support and care for our mother throughout her
remaining life.‖
Integrality
As Mrs Geetha is hemiplegic and ready for discharge, her
family has to do some modifications at home. She has to
get treatment for her HTN and DM also. Her son stated, ―I
do not know how to take care of her at home and prevent
any forth coming problems.‖
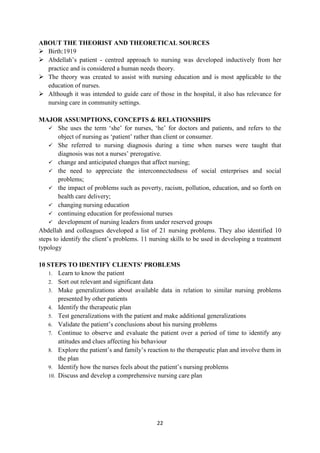
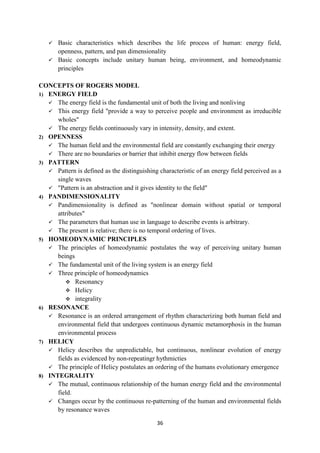
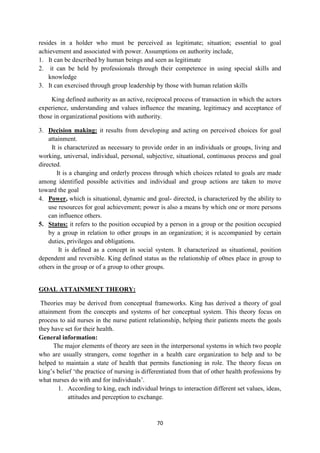
Nursing care plan for Mrs Geetha
Sr.
no.
Nursing
diagnosis
Goal/
objective
Planning Implementation Evaluation
1 Self-care
deficit
related to
immobility
To meet the
self-care
needs
(activities of
daily living
[ADL])
-To assist the
client in meeting
ADL.
-Provide constant
encouragement
-Provide family
support.
-Performed ADL
which the client is
not able to do
-Assisted the client in
washing, eating,
grooming etc.
-Provided constant
Client is
carrying out
the activities
within her
limits.
Family
members are](https://image.slidesharecdn.com/nursing-theories-module-220714121928-db61f884/85/Nursing-Theories-module-pdf-40-320.jpg)





















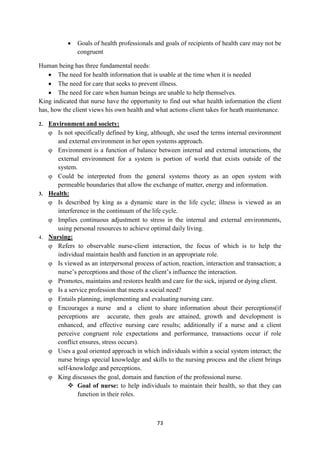







































![128
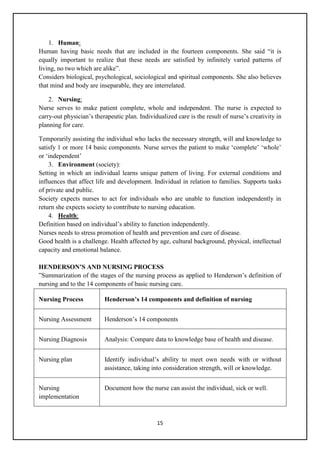
Leininger (1991) identified three nursing decision and action modes to achieve culturally
congruent care.
1. Cultural preservation or maintenance.
2. Cultural care accommodation or negotiation.
3. Cultural care repatterning or restructuring.
MAJOR CONCEPTS [LEININGER (1991)]
Illness and wellness are shaped by a various factors including perception and coping skills, as
well as the social level of the patient.
Cultural competence is an important component of nursing.
Culture influences all spheres of human life. It defines health, illness, and the search for relief
from disease or distress.
Religious and Cultural knowledge is an important ingredient in health care.
The health concepts held by many cultural groups may result in people choosing not to seek
modern medical treatment procedures.
Health care provider need to be flexible in the design of programs, policies, and services to
meet the needs and concerns of the culturally diverse population, groups that are likely to be
encountered.
Most cases of lay illness have multiple causalities and may require several different
approaches to diagnosis, treatment, and cure including folk and Western medical
interventions.
The use of traditional or alternate models of health care delivery is widely varied and may
come into conflict with Western models of health care practice.
Culture guides behavior into acceptable ways for the people in a specific group as such
culture originates and develops within the social structure through inter personal interactions.
For a nurse to successfully provide care for a client of a different cultural or ethnic to
background, effective intercultural communication must take place.
APPLICATION TO NURSING
To develop understanding, respect and appreciation for the individuality and diversity of
patients beliefs, values, spirituality and culture regarding illness, its meaning, cause,
treatment, and outcome.
To encourage in developing and maintaining a program of physical, emotional and spiritual
self-care introduce therapies such as ayurveda and pancha karma.
HEALTH PRACTICES IN DIFFERENT CULTURES
USE OF PROTECTIVE OBJECTS
Protective objects can be worn or carried or hung in the home- charms worn on a string or
chain around the neck, wrist, or waist to protect the wearer from the evil eye or evil spirits.
USE OF SUBSTANCES.
It is believed that certain food substances can be ingested to prevent illness.
E.g. eating raw garlic or onion to prevent illness or wear them on the body or hang them in
the home.](https://image.slidesharecdn.com/nursing-theories-module-220714121928-db61f884/85/Nursing-Theories-module-pdf-128-320.jpg)




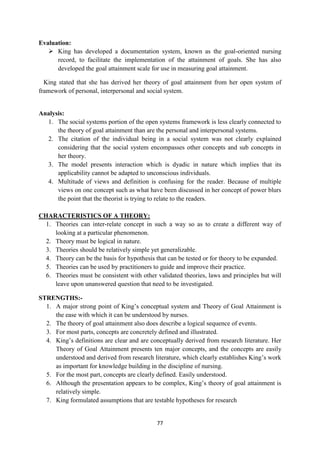
![138
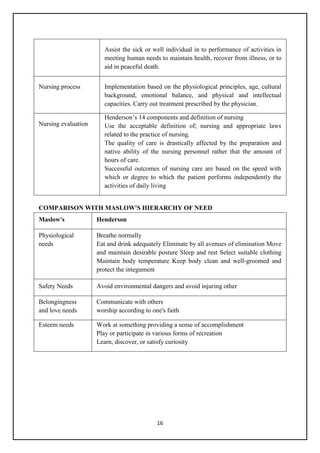
Hildegard. E. Peplau
INTRODUCTION
Theorist -Hildegard. E. Peplau
Born in Reading, Pennsylvania [1909], USA
Diploma program in Pottstown, Pennsylvania in 1931.
BA in interpersonal psychology - Bennington College in 1943.
MA in psychiatric nursing from Colombia University New York in 1947.
EdD in curriculum development in 1953.
Professor emeritus from Rutgers university
Started first post baccalaureate program in nursing
Published Interpersonal Relations in Nursing in 1952
1968 :interpersonal techniques-the crux of psychiatric nursing
Worked as executive director and president of ANA.
Worked with W.H.O, NIMH and Nurse Corps.
Died in 1999.
Theory of interpersonal relations is a middle range descriptive classification theory.
The theory was influenced by Harry Stack Sullivan's theory of inter personal relations (1953).
The theorist was also influenced by Percival Symonds, Abraham Maslow's and Neal Elger
Miller.
Peplau's theory is also refered as psychodynamic nursing, which is the understanding of one‘s
own behavior.
16. PEPLAU'S THEORY OF INTERPERSONAL RELATIONS](https://image.slidesharecdn.com/nursing-theories-module-220714121928-db61f884/85/Nursing-Theories-module-pdf-138-320.jpg)


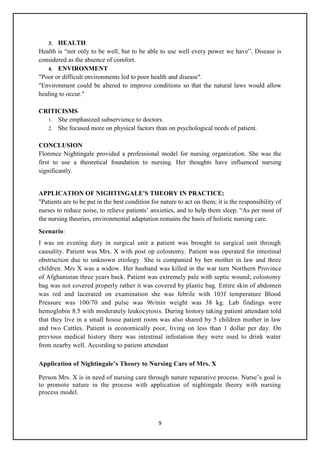
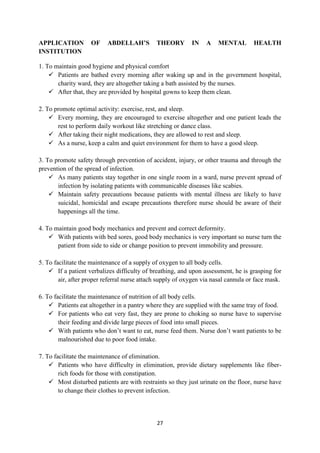
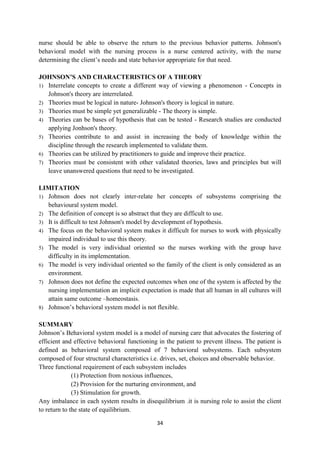
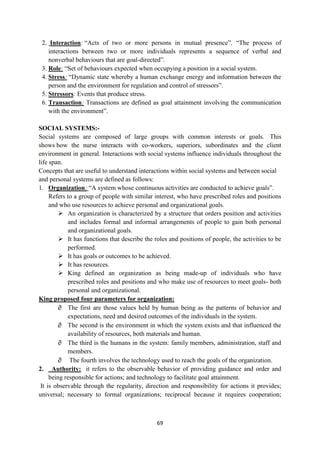
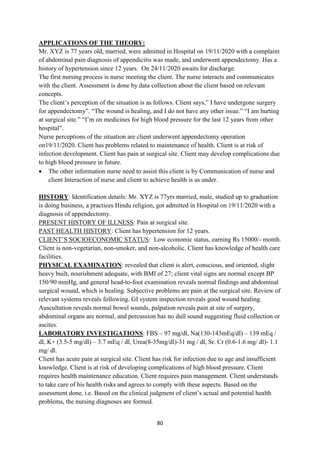
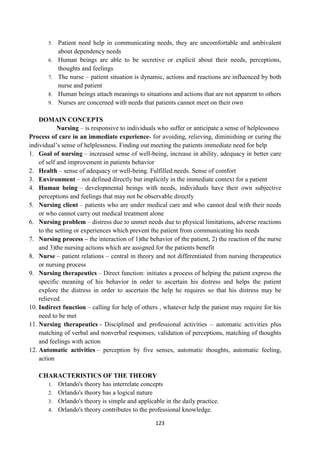
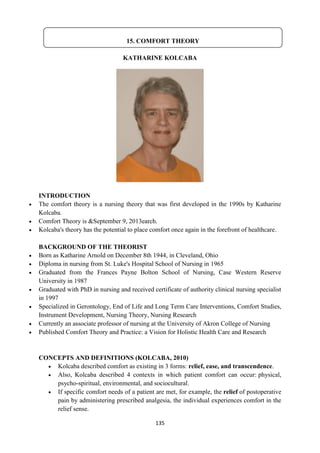
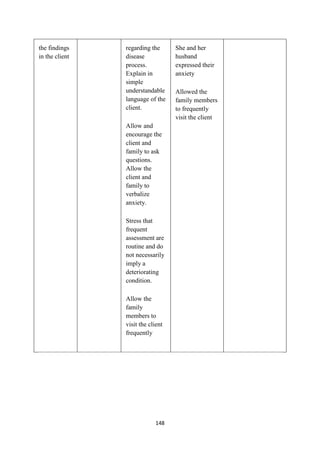
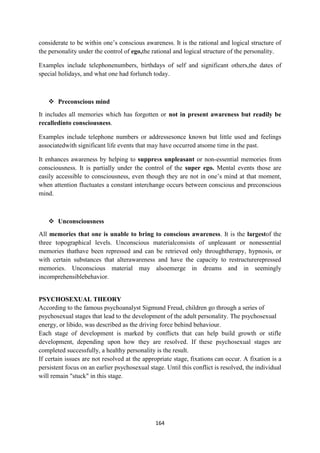
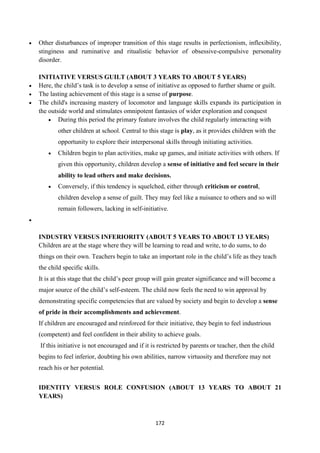
![142
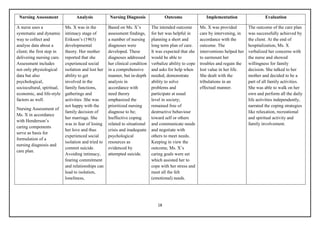
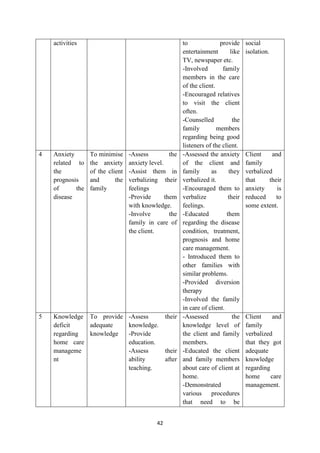
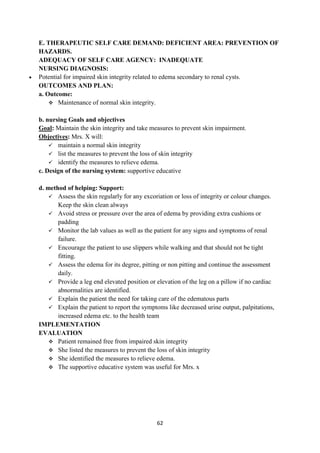
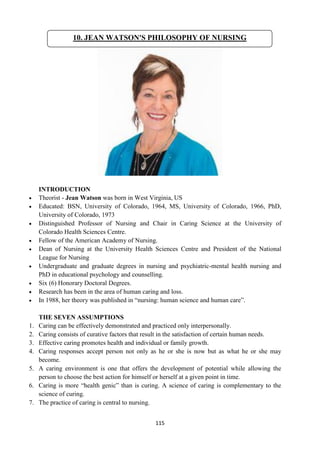
Assessment
Data collection and analysis [continuous]
May not be a felt need
Orientation
Non continuous data collection
Felt need
Define needs
Nursing diagnosis
Planning
Mutually set goals
Identification
Interdependent goal setting
Implementation
Plans initiated towards achievement of
mutually set goals
May be accomplished by patient , nurse or
family
Exploitation
Patient actively seeking and drawing help
Patient initiated
Evaluation
Based on mutually expected behaviors
May led to termination and initiation of new
plans
Resolution
Occurs after other phases are completed
successfully
Leads to termination a relationship
PEPLAU’S WORK AND CHARACTERISTICS OF A THEORY
Interrelation of concepts
Four phases interrelate the different components of each phase.
Applicability
The nurse patient interaction can apply to the concepts of human being, health, environment
and nursing.
Theories must be logical in nature -
This theory provides a logical systematic way of viewing nursing situations
Key concepts such as anxiety, tension, goals, and frustration are indicated with explicit
relationships among them and progressive phases
Generalizability
This theory provides simplicity in regard to the natural progression of the NP relationship.
Theories can be the bases for hypothesis that can be tested
Peplau's theory has generated testable hypotheses.
Theories can be utilized by practitioners to guide and improve their practice.
Peplau‘s anxiety continuum is still used in anxiety patients
Theories must be consistent with other validated theories, laws, and principles but will leave
open unanswered questions that need to be investigated.
Peplau's theory is consistent with various theories](https://image.slidesharecdn.com/nursing-theories-module-220714121928-db61f884/85/Nursing-Theories-module-pdf-142-320.jpg)














































![Peplau theory [version.2]](https://cdn.slidesharecdn.com/ss_thumbnails/peplautheoryv-181019183234-thumbnail.jpg?width=640&height=640&fit=bounds)






































































