The document provides an overview of the male and female reproductive systems. It describes:
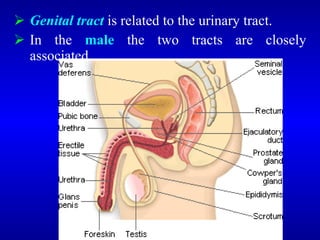
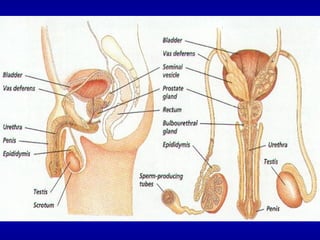
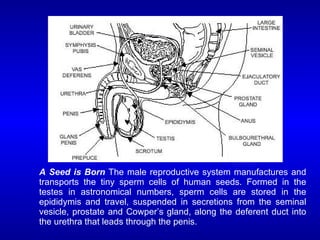
- The structures and functions of the male reproductive organs including the testes, vas deferens, seminal vesicles, prostate gland, and penis.
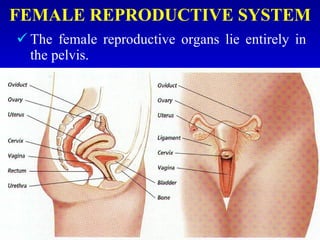
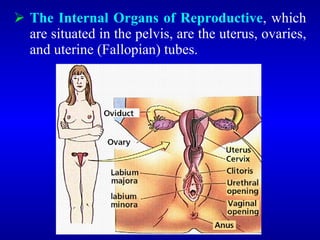
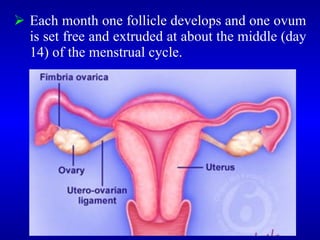
- The structures and functions of the female reproductive organs including the ovaries, fallopian tubes, uterus, vagina, and vulva.
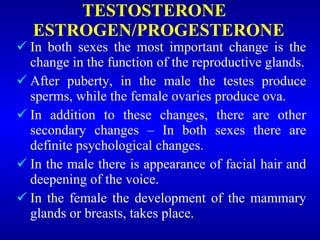
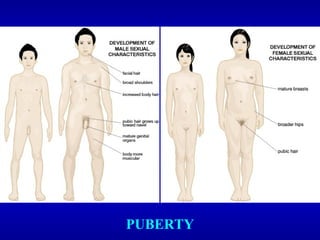
- The hormonal changes that occur during puberty in both sexes to trigger sexual maturation and secondary sex characteristics.
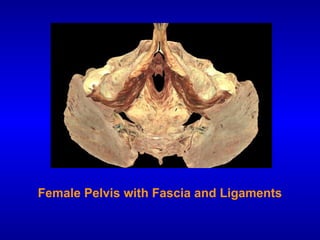
- Similarities and differences between the male and female pelvis and their contents that support reproduction.
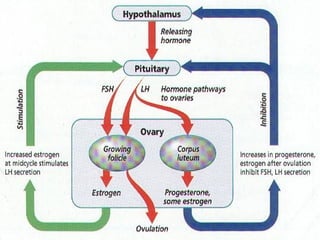

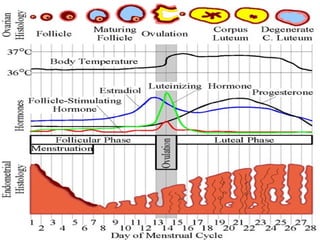
![The ovary has 3 functions
2. The production of ova
3. The production of estrogens
4. The production of progesterone
}Control of
menstruation
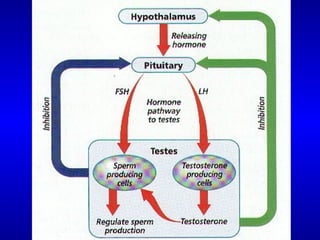
The gonadotrophic hormones of the anterior
pituitary control the production of hormones by
the ovary itself.
Follicle stimulating hormone [FSH] is essential
for the early development of the Graafian
follicle; and the pituitary also controls this
growth by the luteinizing hormone [LH] and the
secretion of the corpus luteum.](https://image.slidesharecdn.com/organs-of-the-reproductive-systemeditedppt4000-221126065705-e41584a5/85/organs-of-the-reproductive-systemeditedppt4000-pdf-53-320.jpg)
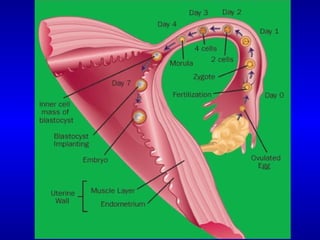
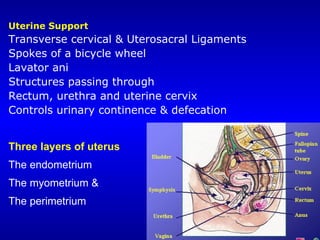
![UTERINE [FALLOPIAN] TUBES
Pass one on each side from the upper angles of the
uterus outwards, in the upper margin of the broad
ligament towards the sides of the pelvis.
They are about 10 cm long, and at their uterine ends
are narrow.
They then enlarge, forming the ampulla, and finally
bend downwards to end in a fimbriated margin.
One of the fimbriae is attacked to the ovary.
In structure the uterine tubes are covered by
peritoneum; beneath this lies the muscular coat of
longitudinal and circular fibers.
The tubes are lined by ciliated epithelial cells.](https://image.slidesharecdn.com/organs-of-the-reproductive-systemeditedppt4000-221126065705-e41584a5/85/organs-of-the-reproductive-systemeditedppt4000-pdf-68-320.jpg)