This document discusses blood pressure measurement and hypotension/hypertension. It provides details on:
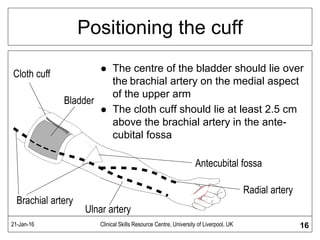
- The importance of accurately measuring blood pressure to assess conditions like hypotension and hypertension.
- The causes and symptoms of hypotension, including postural hypotension. Postural hypotension is a drop in blood pressure when moving from lying to standing.
- The causes and types of hypertension, including primary/essential hypertension which has no identifiable cause, and malignant hypertension which is a medical emergency.