Downloaded 22 times






















![Questions? General Questions: Martha Quinn [email_address] Questions on Dallas or Chicago Initiatives: Darla Williams [email_address] Technical Questions: Gillian Mayman [email_address]](https://image.slidesharecdn.com/policywebinar-110628080916-phpapp01/85/Organizational-Policy-and-Systems-Change-58-320.jpg)

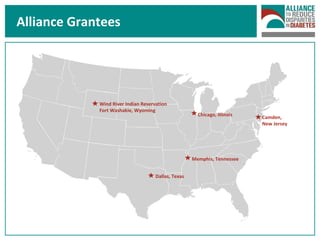
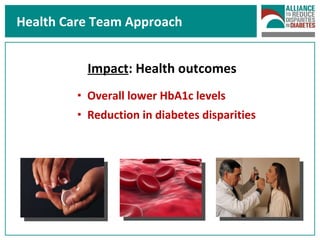
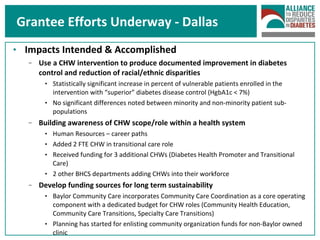
The document discusses the importance of organizational policy and systems change, particularly in the context of diabetes care across various locations, including Dallas and Chicago. It highlights examples of successful systems changes through community health workers and clinic redesigns, emphasizing the positive impacts on health outcomes and disparities. The overarching goal is to create sustainable policies that improve chronic disease management and support historically underserved populations.









































































































