This document provides information on various oral red lesions, including their etiology, clinical presentation, diagnosis, differential diagnosis, and prognosis. It describes conditions such as ecchymosis, erythroplakia, fissured tongue, hemangioma, hereditary hemorrhagic telangiectasia, petechiae, plasma cell gingivitis, pyogenic granuloma, varices, and Kaposi's sarcoma. For each lesion, it outlines the potential causes, common signs and symptoms, diagnostic process, important distinctions from other diseases, and typical outlook. The goal is to educate medical professionals on interpreting and managing different types of red lesions in the oral cavity.




















![Petechiae
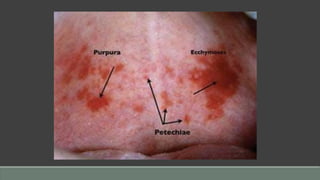
Definition: Petechiae are pinpoint hemorrhages that occur in subcutaneous or submucosal
tissues in a wide variety of conditions. Because of their diversity, the differential diagnosis of
oral mucosal petechial hemorrhages is complex.
Etiology
• Viral infection (Epstein-Barr virus [EBV]-mononucleosis; measles), rickettsial infection
• Thrombocytopenia, leukemia
• Disseminated intravascular coagulation (DIC)
• Trauma: prolonged coughing, frequent vomiting, giving birth, violent Valsalva maneuvers](https://image.slidesharecdn.com/4oralredlesionsgui-230809194514-a7e2ff25/85/Oral-Red-Lesions-pdf-48-320.jpg)










![Kaposi’s Sarcoma
Etiology
• Several forms
◦ • Classic idiopathic form affecting extremeties
◦ • Endemic form (African)
◦ • Immunosuppression-associated form
◦ • Acquired immunodeficiency syndrome (AIDS)-associated form
• All forms, especially AIDS-associated and immunosuppressionassociated forms, may be
caused by or closely related to a herpesvirus (human herpesvirus 8 [HHV-8] or Kaposi’s
sarcoma–associated herpesvirus [KSHV]).](https://image.slidesharecdn.com/4oralredlesionsgui-230809194514-a7e2ff25/85/Oral-Red-Lesions-pdf-73-320.jpg)



































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)



