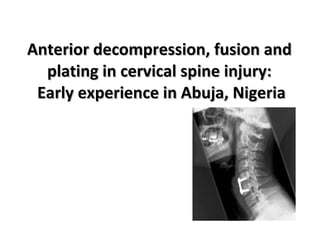
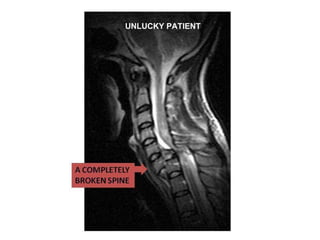
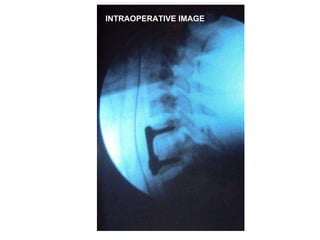
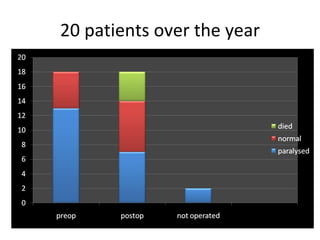
The document discusses cervical spine injuries and cervical spondylotic myelopathy. It presents early experience with anterior decompression, fusion and plating for cervical spine injuries in Abuja, Nigeria. It describes surgical techniques used including anterior cervical discectomy and fusion. It highlights the importance of early referral for surgery and discusses challenges including lack of intensive care and rehabilitation facilities.
























![Safe surgical dislocation[ssd] for avascular necrosis hip[ avn]](https://cdn.slidesharecdn.com/ss_thumbnails/safesurgicaldislocationssdforavascularnecrosishipavn-200914081007-thumbnail.jpg?width=640&height=640&fit=bounds)









































