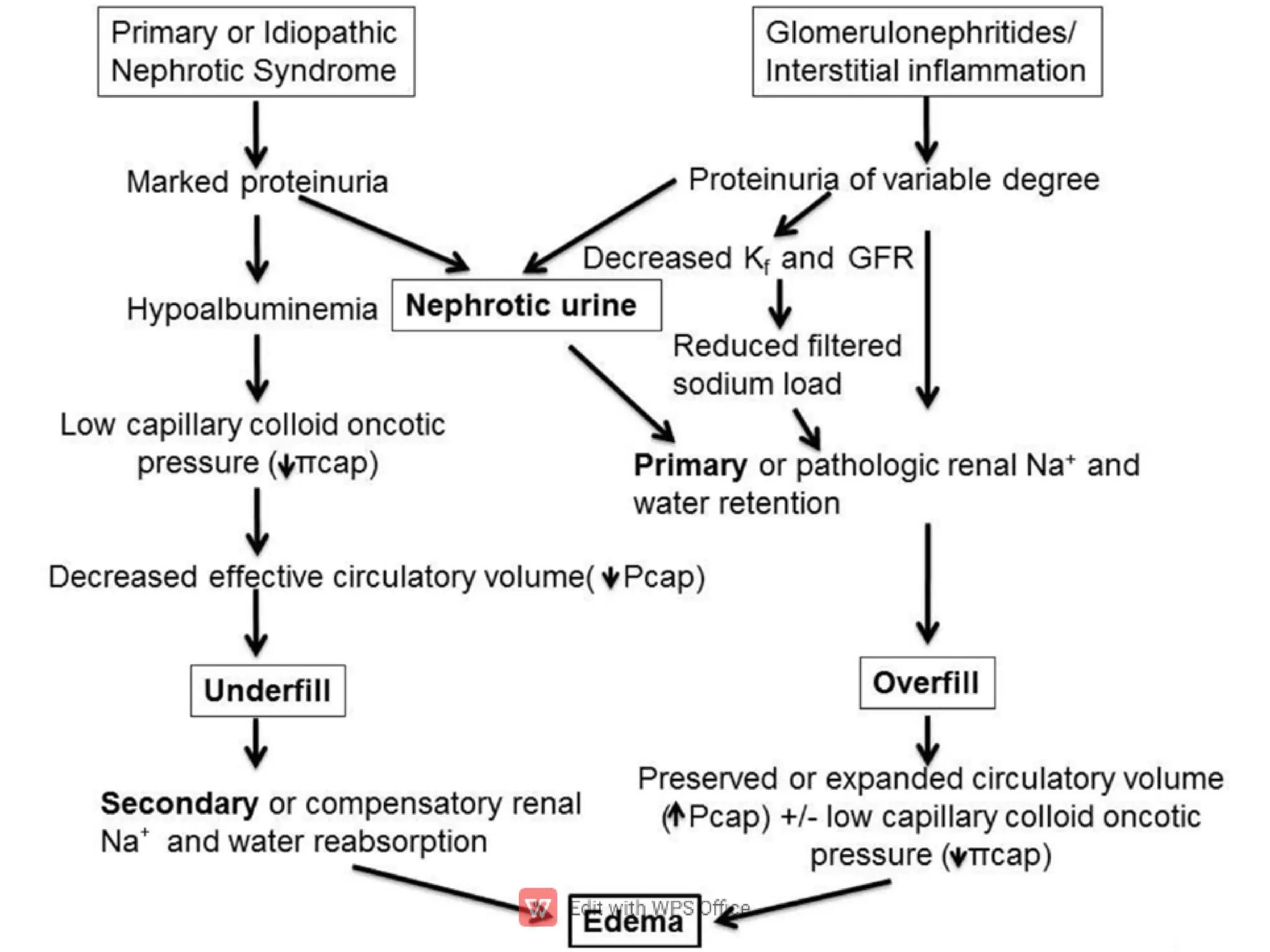
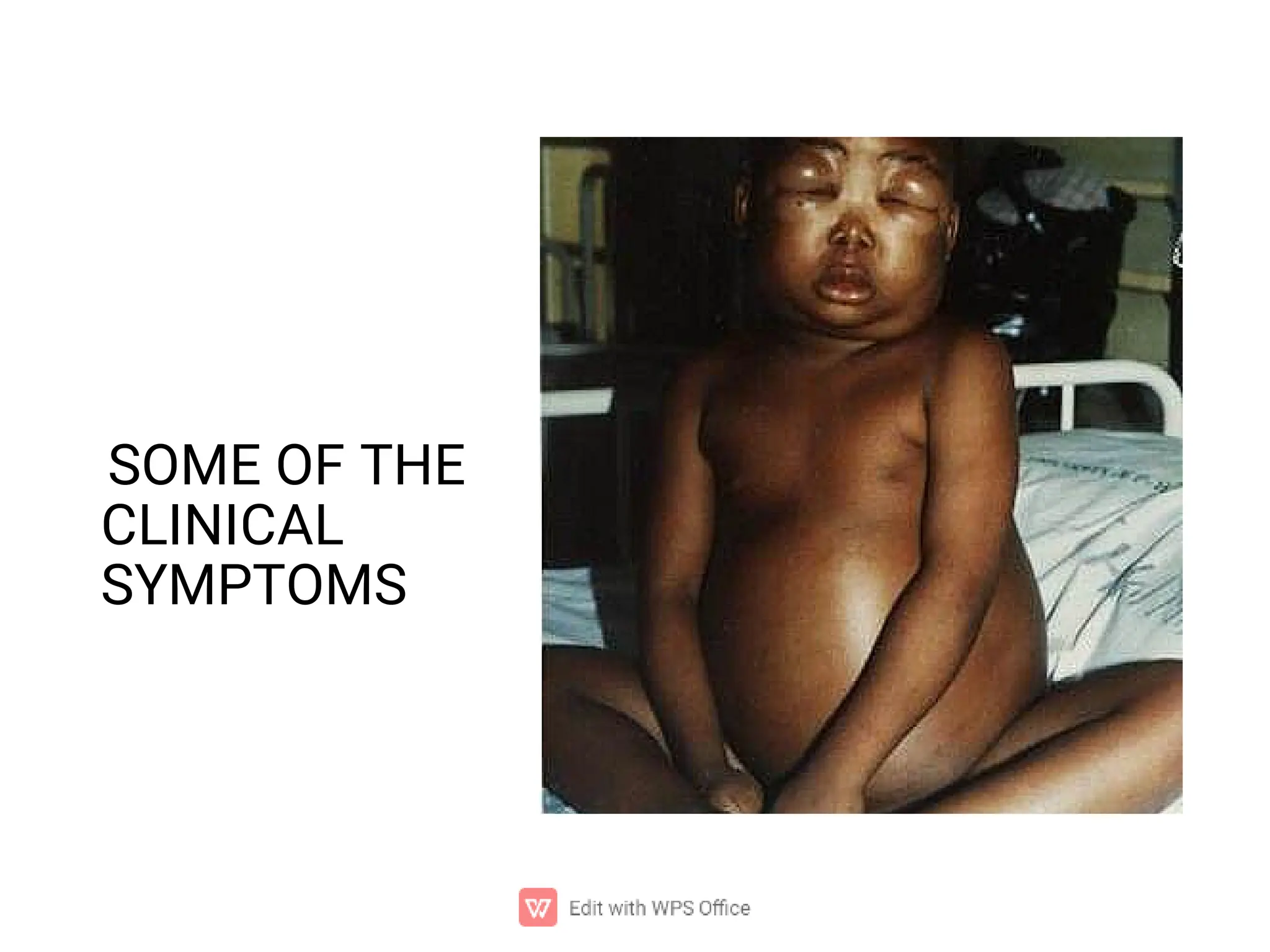
The document presents a seminar on nephrotic syndrome, detailing its definition, incidence, causes, pathophysiology, clinical manifestations, diagnostic evaluation, and management strategies. It emphasizes the condition's impact on children, particularly between ages 2-6, and outlines both medical and nursing management approaches, including corticosteroid therapy and monitoring of fluid balance. Prognosis varies, with steroid-responsive cases having a good outcome, while steroid-resistant cases have a poorer prognosis.




























![Nephrotic syndrome [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/nephroticsyndromeautosaved-200124152149-thumbnail.jpg?width=640&height=640&fit=bounds)



















