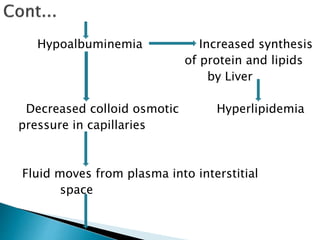
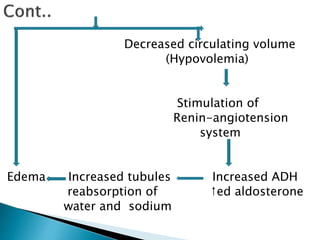
Childhood nephrotic syndrome is a kidney condition characterized by significant protein loss in the urine, leading to symptoms such as edema, hyperlipidemia, and hypoalbuminemia, predominantly affecting children aged 2-5, especially males. Causes may be primary, such as minimal change nephropathy, or secondary, associated with infections, toxins, or systemic diseases, and the condition can vary in types based on age and etiology. Management includes bed rest, dietary modifications, steroid therapy, and potential diuretics or immunosuppressive drugs, alongside careful monitoring of the child's symptoms and nutritional status.