Introduction
• Nephrotic syndromeisn't a disease but is a
condition Cxtxd by marked proteinuria,
hypoalbuminemia, hyperlipidemia, lipiduria,
increased coagulation, & edema.
• It results from a glomerular defect that affects
the vessels' permeability & indicates renal
damage.
• Some forms of nephrotic syndrome may
eventually progress to end-stage renal failure.
Nephrotic Syndrome
Nephrotic Syndrome
•Chronic renal
disorder in
which the
basement
membrane
surfaces of the
glomeruli are
affected, cause
loss of protein
in the urine.
5.
Nephrotic criteria
1. Massiveproteinuria:
• Qualitative proteinuria: 3+ or 4+,
• Quantitative proteinuria : more than 40
mg/m2/hr in children (selective).
2. Hypo-proteinemia : total plasma proteins <
5.5g/dl & serum albumin : < 2.5g/dl.
3. Hyperlipidemia: Serum cholesterol : >
5.7mmol/L
4. Edema: pitting edema in different degree
Types
1. Idiopathic nephriticsyndrome
– The most common in children for about
90%
2. Congenital Nephrotic Syndrome
– Rare in children & congenital
– It is inherited by an autosomal recessive
gene, meaning that males & females are
equally affected
8.
Pathophysiology
I. Proteinuria :Increaseglomerular permeability for
proteins due to loss of negative charged
glycoprotein
• Degree of protineuria:-
– Mild: less than 0.5g/m2/day
– Moderate: 0.5 – 2g/m2/day
– Severe: more than 2g/m2/day
• Type of proteinuria:-
A-Selective proteinuria: where proteins of low
molecular weight, such as albumin, are excreted
more readily than protein of HMW
B-Non selective : LMW+HMW are lost in urine
9.
Pathophysiology /2
II. Hypoalbinaemia
Dueto hyperproteinuria----- Loss of plasma
protein in urine mainly the albumin.
Increased catabolism of protein during acute
phase.
Signs & symptoms
1.Mainmanifestations:
Edema (varying degrees) is the common
symptom
Local edema: edema in face , around
eyes( Periorbital swelling) , in lower
extremities.
Generalized edema (anasarca), edema
in penis and scrotum.
14.
The symptoms ofnephrotic syndrome
• Fatigue & malaise . Decreased appetite
• Weight gain from excess fluid
• Dull hair
• Foamy urine, decrease in frequency of urination
• Pale fingernail beds .
• Ears cartilage may feel less firm
• Food intolerances or allergies
• Proteinuria, high levels
• Low levels of proteinemia due to its loss in the
urine
• High cholesterol levels in the blood
16.
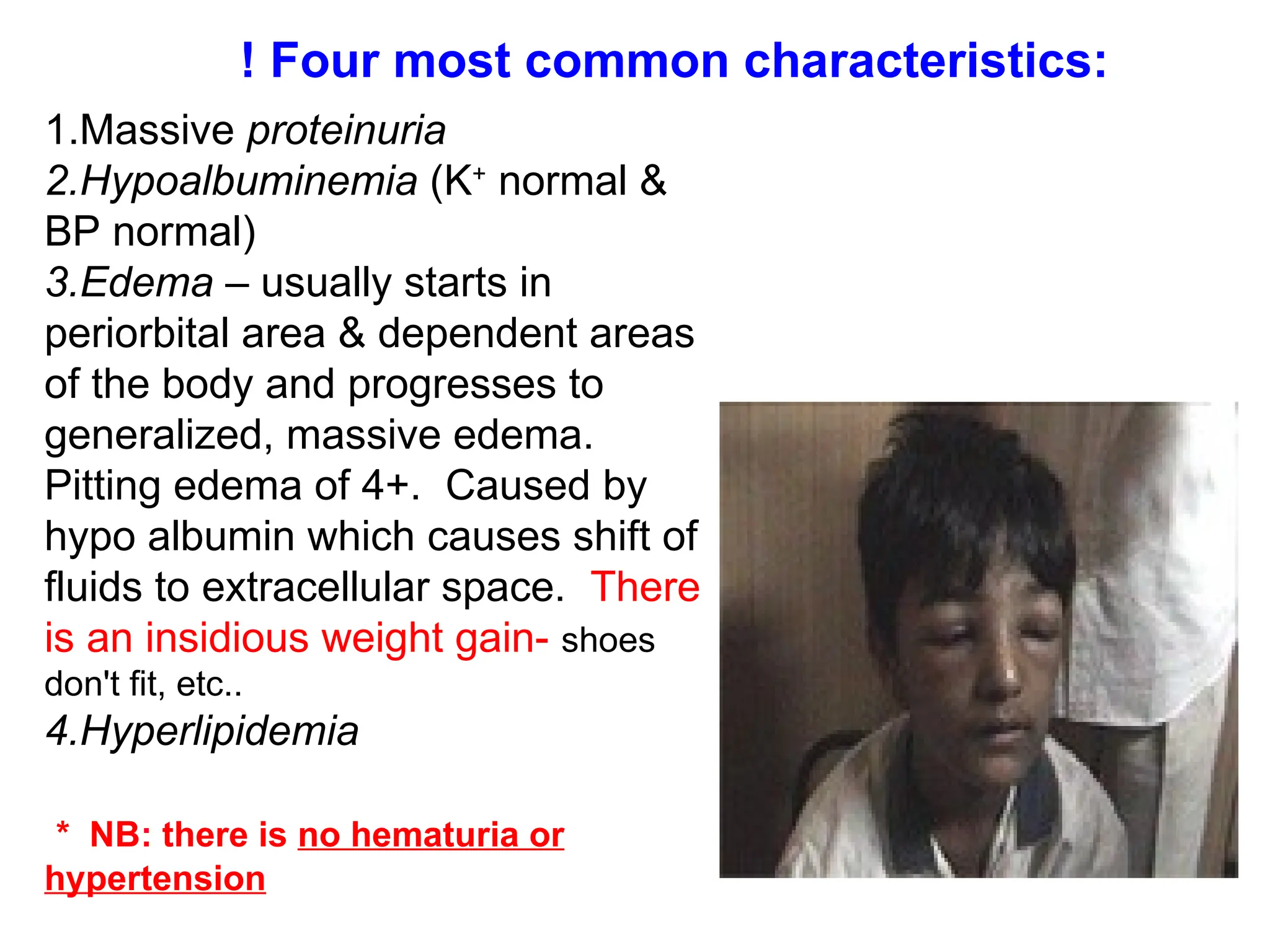
1.Massive proteinuria
2.Hypoalbuminemia (K+
normal&
BP normal)
3.Edema – usually starts in
periorbital area & dependent areas
of the body and progresses to
generalized, massive edema.
Pitting edema of 4+. Caused by
hypo albumin which causes shift of
fluids to extracellular space. There
is an insidious weight gain- shoes
don't fit, etc..
4.Hyperlipidemia
* NB: there is no hematuria or
hypertension
! Four most common characteristics:
17.
Diagnosis
• Urine tests(to check for protein)
>40mg/m2/hr
• Blood tests for levels of cholesterol & albumin
• Renal ultrasound.
• Renal biopsy
18.
Blood specimen
• Serumprotein: decrease >5.5gm/dL ,
Albumin levels are low ( < 2.5gm/dL).
• Serum cholesterol & triglycerides:
Cholesterol > 5.7mmol/L (220mg/dl).
• ESR↑ > 100mm/hr during activity phase
• Serum complement: Vary with clinical type.
• Renal function
Nrsg care
1. Assessand Document the location and
character of the patient's edema.
2. Vital signs: BP, Pulse
3. Monitor & record intake and output & weigh
the patient accurately each morning after s/he
voids & before S/he eats. Make sure S/he's
wearing the same amount of clothing each time
you weigh him/her.
4. Careful monitoring of IV fluids
5. Plan a low-sodium diet with moderate amounts
of protein.
6. Frequently check urine for protein.
21.
Nrsg care
7. Monitorplasma albumin & transferrin
concentrations to evaluate overall nutritional
status.
8. Provide meticulous skin care
9. Use a reduced-pressure mattress or padding to
help prevent pressure ulcers.
10. To prevent the occurrence of thrombophlebitis,
encourage activity & exercise
11. Psychological care - Give the patient & family
reassurance & support
12. Provide appropriate provisions corticosteroids
13. Give diuretic if prescribed
22.
Complications
1. Infections: Infectionsis a major complication in
children with NS. It frequently trigger relapses.
Common infections: URI, peritonitis, cellulitis &UTI
2. Hypercoagulability (Thrombosis)
3. Cardiovascular disease :-Hyperlipidemia, may
be a risk factor for cardiovascular disease.
4. Hypovolemic shock
5. Others: growth retardation, malnutrition, adrenal
cortical insufficiency





























![Nephrotic_Syndrome[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/nephroticsyndrome1-220824090858-5a841ab2-thumbnail.jpg?width=640&height=640&fit=bounds)





































