Download as PDF, PPTX








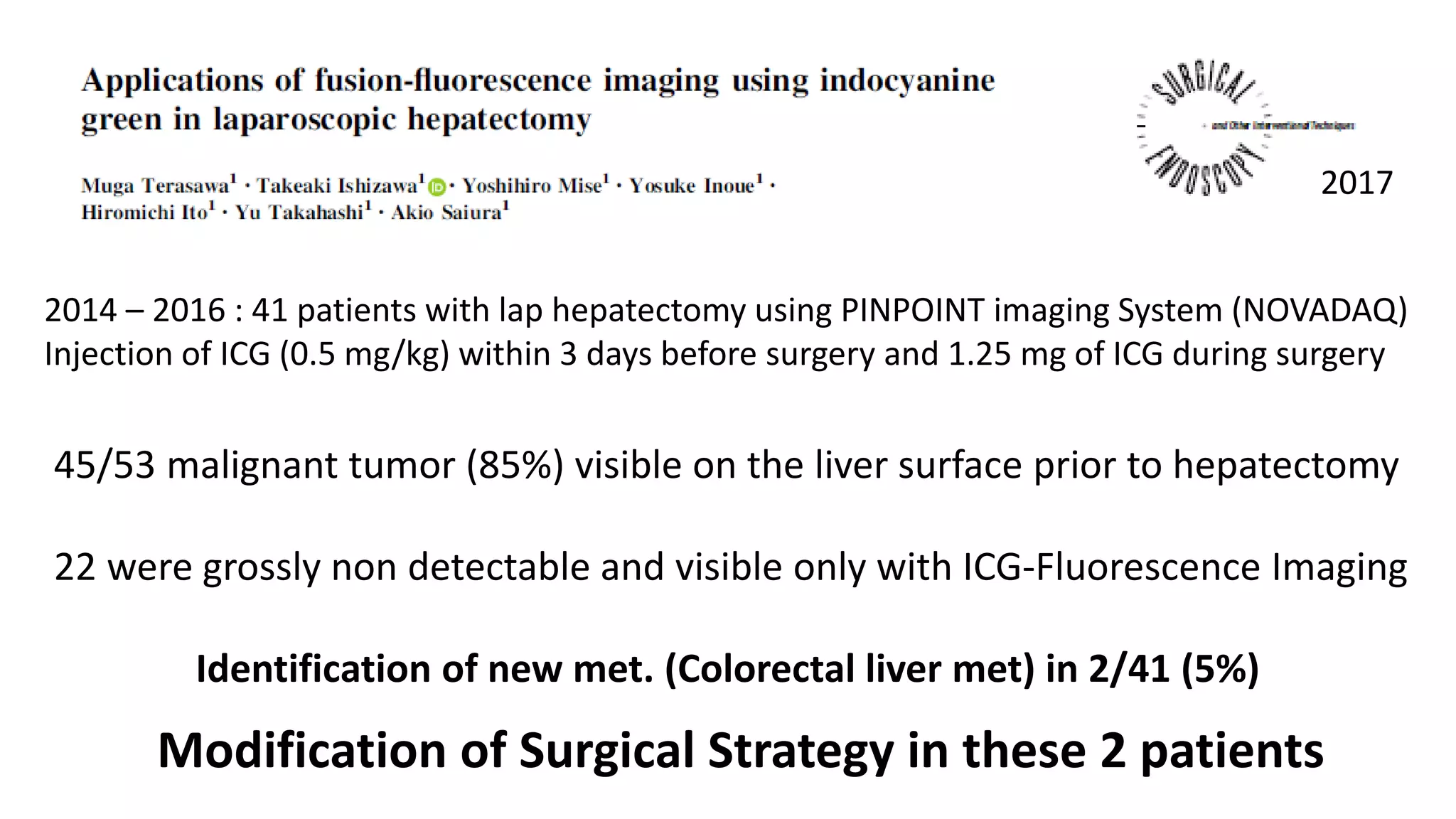


















This document discusses new technologies that can help overcome drawbacks of laparoscopic liver surgery. It describes how fluorescent imaging agents like indocyanine green can help identify subcapsular tumors and margins not visible to the naked eye. Studies showed this approach detected additional tumors in a percentage of cases. Robotic assistance and intraoperative pathological analysis using confocal microscopy may also help improve visualization and margin assessment. Synergic robots that guide the surgeon's movements could help compensate for limitations of laparoscopic instruments. These techniques aim to enhance laparoscopic liver surgery and make it a safer alternative to open surgery.





































![Hepatic Resection techniques[Autosaved]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hepaticresectionautosaved-1-240310100405-b4ce2794-thumbnail.jpg?width=640&height=640&fit=bounds)















































