Downloaded 19 times

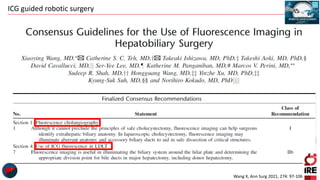

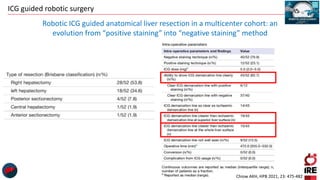

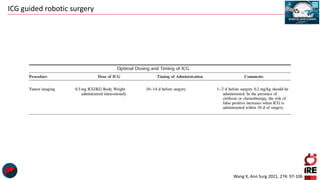
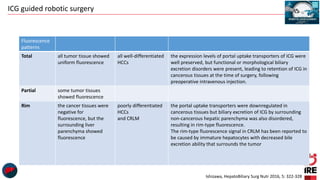
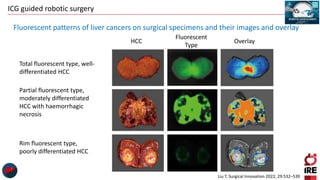
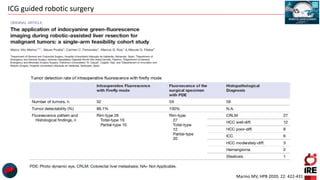






The document discusses the use of indocyanine green (ICG) in robotic hepato-biliary-pancreatic surgery, detailing its applications in liver cancer surgeries and the benefits of robotic and fluorescence-guided techniques. It highlights ICG's implications for improving surgical visualization, detecting tumors, and enhancing patient outcomes while addressing challenges such as imaging limitations and the need for further technological advancements. The summary also notes that future developments must align with clinical needs and aim for practical applications in surgery.























































































