The document discusses the transformation of healthcare in the Asia-Pacific region driven by the COVID-19 pandemic, emphasizing the shift toward digital health technologies and patient-centric care. It highlights the need for medtech innovation and collaboration to improve health outcomes and address increased demands for remote care. Furthermore, the document includes insights from Ashley McEvoy of Johnson & Johnson on how these changes impact the healthcare landscape and medtech's future.






















![30 ASIAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE - 55, 2022
vasodilated and dysautoregulated. In this
regard, they cannot further vasodilate
in response to increased carbon dioxide
tension from diuretic acetazolamide, a
carbonic anhydrase inhibitor.
Quantitative MR angiography
(q-MRA)’s non-invasive optimal vessel
analysis (NOVA) is also essential to
quantify and measure blood flow
through large vessels of the Circle of
Willis (Figure 3b). Together with formal
cerebral angiography, it can be used to
estimate pial and collateral flow. It gives
reasonable estimates of augmentable
flow to ensure appropriate blood
velocity ranges after bypass, and also in
anticipation of longer term collateral
shift, cerebral blood flow re-organisation.
Surgical procedure
Direct superficial temporal artery
(STA) [donor] and middle cerebral
artery (MCA) M4 cortical branch
[recipient] bypass is generally
preferred. Meticulous attention to
blood pressure control, maintenance
of intravascular volume and depth
of anaesthesia are essential to avoid
cerebral hypoperfusion during these
cases with underlying steno-occlusive
disease. Intraoperative end-to-side
anastomoses are performed using 10-0
nylon sutures with indocyanine green
(ICG) and intra-operative angiographic
confirmation of anastomotic patency.
Individualised blood pressure goals
with gradual liberalisation of these
parameters are done post-operatively
with continuation of antithrombotic
agents to maintain anastomotic patency
and to avoid reperfusion-related injury.
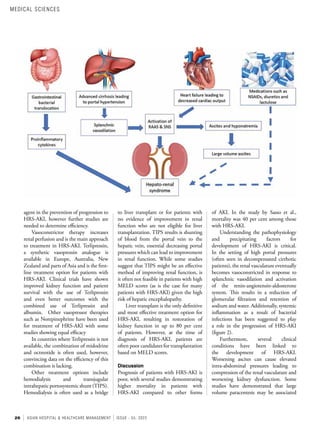
Conclusion
For patients who have been medically
optimised but still at risk of ischemic
symptoms of haemodynamic
insufficiency due to steno-occlusive
cerebrovascular disease, one can identify
candidateswithreversiblehypoperfusion,
exhausted autoregulation and impaired
vasodilatory reserve. Consideration
of extracranial-intracranial bypass
Artery Normal Mean Flow Velocity [MFV]
(cm/s)
ICA Siphon < 70
MCA M1-M2 < 80
ACA A1 < 80
BA < 50
VA < 60
PCA < 50
Arterial Stenosis (50 per cent) Mean Flow Velocity [MFV] (cm/s)
ICA Siphon, ACA (A1) < 90
MCA M1-M2 < 100
BA-VA-PCA < 70
Figure 1. Stages of Cerebral Hypoperfusion.
Table 1. Cerebrovascular mean flow velocities.
ICA = internal carotid artery, MCA = middle cerebral artery, ACA = anterior
cerebral artery, BA = basilar artery, VA = vertebral artery, PCA = posterior
cerebral artery.
procedure can be reliably made to
identify patients who have reasonable
chances of augmentable flow-induced
long-term cerebral flow re-organisation
while preventing future hypoperfusion
events. Identification of these candidates
are made after medical optimisation,
including blood pressure management,
antithrombotic therapy and treatment
of underlying brain-body interactions
targeted at optimising cerebral blood
flow and oxygen delivery.
MEDICAL SCIENCES](https://image.slidesharecdn.com/ahhm-issue-55-220209071453/85/New-Normal-New-Future-Free-Download-E-book-32-320.jpg)