NEONATAL POLYCYTHEMIA
Polycythemia —Polycythemia is defined as hematocrit (HCT) or hemoglobin (HGB) level above the
upper limit of normal (>2 standard deviations) for gestational and postnatal age .
In term newborns, the upper limits for HCT and HGB values differ depending upon the type of blood
sample:
●For peripheral venous blood samples, the upper limit for HCT is 65 percent and for HGB is 22 g/dL
●For capillary blood samples, the upper limit for HCT is 75 percent and for HGB is 23.7 g/dL
3.
term newborns havean increased red cell mass caused by the fetal response of
increased hemoglobin production to a relatively hypoxic intrauterine
environment and possibly vasomotor instability and venous pooling in the
newborn immediately after birth.
The hematocrit (HCT) increases after birth, reaching a maximum at
approximately two hours of age, then decreases to levels in cord blood by 18
hours of age
4.
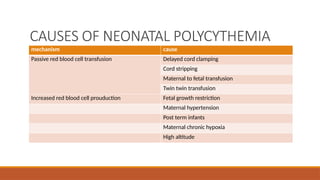
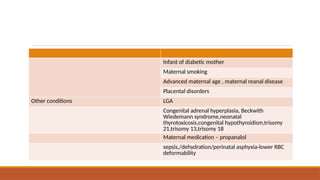
CAUSES OF NEONATALPOLYCYTHEMIA
mechanism cause
Passive red blood cell transfusion Delayed cord clamping
Cord stripping
Maternal to fetal transfusion
Twin twin transfusion
Increased red blood cell prouduction Fetal growth restriction
Maternal hypertension
Post term infants
Maternal chronic hypoxia
High altitude
CLINICAL FEATURES
Asymtamatic (onlyplethora)
Central nervous system :
Early : Hypotonia and sleepiness, irritability, jitteriness, seizures and infarcts,
cerebral venous sinus thrombosis.
Late : motor deficits, lower achievement and IQ scores.
Metabolism
hypoglycaemia, Jaundice, Hypocalcemia
HYPOGLYCEMIA _ increasedglucose utilization by the increased number of
circulating red cells. and hypoglycemia in these infants may be related to
underlying causes of polycythemia
Hyperbilirubinemia — At least one-third of infants with polycythemia develop
hyperbilirubinemia , most likely due to the breakdown of an increased number
of circulating red cells
11.
Diagnosis
Who to test—
Eligible candidates
Small for gestational age
Large for gestational age
Monochorionic twins (larger twin)
Infant with morphological features of IUGR
12.
Schedule
2hr of life;if high, repeat at 6hr,12hr,24hr and 48 hr.
Method
Centrifuge venous blood in heparinized capillaries for 3to 5 minutes @ 10000
to 15000rpm .
13.
Laboratory testing
Pitfalls oftesting –
•Type of blood sample – HCT values are highest in capillary samples,
intermediate in peripheral venous samples, and lowest in samples drawn from
the umbilical vein
•Age at the time of sampling – The HCT increases after birth, reaching a
maximum at approximately two hours of age, then decreases to levels in cord
blood by 18 hours of age].
•Method of HCT measurement – Values obtained from centrifuged samples are
higher than those using cell counters and correlate better with blood viscosity .
14.
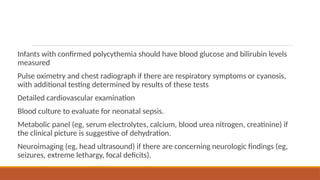
Infants with confirmedpolycythemia should have blood glucose and bilirubin levels
measured
Pulse oximetry and chest radiograph if there are respiratory symptoms or cyanosis,
with additional testing determined by results of these tests
Detailed cardiovascular examination
Blood culture to evaluate for neonatal sepsis.
Metabolic panel (eg, serum electrolytes, calcium, blood urea nitrogen, creatinine) if
the clinical picture is suggestive of dehydration.
Neuroimaging (eg, head ultrasound) if there are concerning neurologic findings (eg,
seizures, extreme lethargy, focal deficits).
15.
Management
Neonate with symptomsof polycythemia is to determine if there is another
underlying cause and to treat that effectively.
Hypoglycemia – monitoring of blood glucose.
Hyperbilirubinemia- monitoring
16.
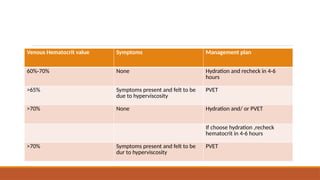
Venous Hematocrit valueSymptoms Management plan
60%-70% None Hydration and recheck in 4-6
hours
>65% Symptoms present and felt to be
due to hyperviscosity
PVET
>70% None Hydration and/ or PVET
If choose hydration ,recheck
hematocrit in 4-6 hours
>70% Symptoms present and felt to be
dur to hyperviscosity
PVET
17.
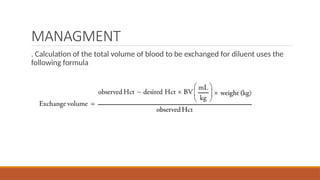
MANAGMENT
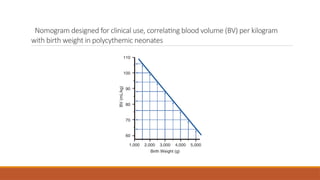
. Calculation ofthe total volume of blood to be exchanged for diluent uses the
following formula
18.
Nomogram designed forclinical use, correlating blood volume (BV) per kilogram
with birth weight in polycythemic neonates
19.
•Either 5% albuminor normal saline (NS) should be used with most institutions
using NS.
•The goal hematocrit should be 50% to 60%.
•. Blood may be removed via an umbilical arterial catheter, umbilical venous
catheter, or peripheral arterial catheter
• NS may be infused via a peripheral or central venous catheter.
20.
Complications of PVET
Hypoglycemia(most common)
Bradycardia
Apnea
Catheter-related complications
Thrombocytopenia
Hypocalcemia
Hypokalemia
Nec
Cardiovascular collapse, sepsis, and pulmonary hemorrhage
21.
Outcomes
Performing a PVETwill decrease the hematocrit and blood viscosity and may
reverse many of the physiologic abnormalities associated with polycythemia.
However, performing a PVET does not appear to change long-term neurologic
Outcomes.
![Laboratory testing
Pitfalls of testing –
•Type of blood sample – HCT values are highest in capillary samples,
intermediate in peripheral venous samples, and lowest in samples drawn from
the umbilical vein
•Age at the time of sampling – The HCT increases after birth, reaching a
maximum at approximately two hours of age, then decreases to levels in cord
blood by 18 hours of age].
•Method of HCT measurement – Values obtained from centrifuged samples are
higher than those using cell counters and correlate better with blood viscosity .](https://image.slidesharecdn.com/neonatalpolycythemia-260119093452-20401a50/85/NEONATAL-POLYCYTHEMIA-pptx-13-320.jpg)




































![Circle of willis (finql)[1].pptx anatomy](https://cdn.slidesharecdn.com/ss_thumbnails/circleofwillisfinql1-250913015401-7ca582c5-thumbnail.jpg?width=640&height=640&fit=bounds)




















