Myoma uteri presentation
•Download as PPTX, PDF•
6 likes•10,003 views

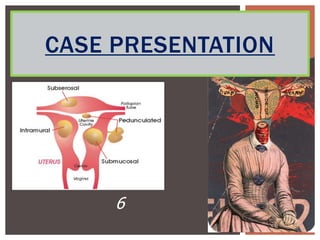
The document describes a case of a 48-year-old Thai woman who presented with abnormal uterine bleeding, anemia, and an abdominal mass found to be multiple uterine fibroids. She underwent a total abdominal hysterectomy with bilateral salpingooophorectomy to treat the fibroids, and her postoperative recovery was uneventful.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Myoma uteri presentation
Similar to Myoma uteri presentation (20)
Myoma uteri presentation
- 1. CASE PRESENTATION 6
- 2. CASE Case 48 10 2555 30 90%
- 3. CHIEF COMPLAINT 5 PTA
- 4. PRESSENT ILLNESS 5 PTA 3 5 8 6-7 2 PTA DMPA
- 6. PAST HISTORY U/D Thyroid 6 PTA P3003 last 20 LMP 4-8 55 (5 days/28-30 days/ 3pads per day) PMP
- 9. PHYSICAL EXAMINATION Vital signs BP 110/50 mmHg PR 72 /min RR 18 /min BT 37 c GA Good consciousness, mild pale, no jaundice, no cyanosis, no edema HEENT Mile pale conjunctivae, no icteric sclerae Cardiovascular Pulse full and regular, normal S1S2, no murmur
- 10. PHYSICAL EXAMINATION Lung Equal chest expansion, clear, no adventitous sound Abdomen No distention, Normoactive bowel sound, soft,, palpable midline pelvic mass size 2/3> PS, globular shape, irregular surface, rubbery, not tender, movable no rebound tenderness Neurological Grossly intact Extremities No edema, no fracture
- 11. PHYSICAL EXAMINATION Per vagina examination : MIUB - Normal Vg - No discharge, no lesion Cx - No mass and polyps, closed Ut - 16 wk. size with globular mass at fundus Adn - No palpable mass, no tenderness CDS - No bulging
- 12. PERTINENT FINDING An middle aged Thai woman 48 years Perimenopausal period Abnormal uterine bleeding Abdominal mass Anemic symptoms Underlying Thyroid disease (Clinical Euthyroid) s/p Surgery 6 years PTA
- 13. PROBLEM LIST Abdominal mass with Abnormal uterine bleeding and anemic symptoms Underlying Thyroid disease Clinical euthyroid s/p Surgery 6 years PTA
- 14. APPROACH AUB
- 15. APPROACH AUB
- 17. DIFFERENTIAL DIAGNOSIS Uterus mass (leiomyoma vs leiomyosarcoma) Adenomyosis Ovarian tumor Endometrium disease Cervical cancer Systemic conditions Hypothyroid Coagulopathies
- 18. INVESTIGATION CBC Hb 10.0 g/dl WBC 6,500 /ul HCT 29.0 % PMN 58.0 % MCV 55.0 fl Lymp 39.0 % MCH 19. pg Mono 1.0 % MCHC 35.1 g/dl Eo 2.0 % Plt 208,000 /ul Baso 0 %
- 19. INVESTIGATION PBS RBC Morphology Abnormal RBC Microcytic 1+ Hypochromic 1+ Target cell, schitocyte Few Thyroid function test FT3 2.245 (1.21-4.18) mmol/l FT4 14.25 (7.2-17.2) mmol/l
- 20. INVESTIGATION UA Color/Appearance Y/C pH 7 Ketone Neg Protein Neg Nitrite Neg Glucose Norm WBC 0-1 RBC 0-1 Sq.epithelium 10-20 Bacteria -
- 21. INVESTIGATION Coagulogram normal BS 86 mg/dl BUN 10 mg/dl Creatinine 0.7 mg/dl Anti-HIV negative CXR normal EKG normal sinus rhythm, rate 70/min
- 22. INVESTIGATION PAP smear Negative for intraepithelial lesion or malignancy but reactive cellular change associate with inflammation Endometrium Biopsy Inactive endometrium
- 24. TREATMENT (11/12/2555) Total abdominal hysterectomy with bilateral salpingooophorectomy Uterus 16 wk size with large intramural myoma at fundus 8x8 cm. and intramural myoma 4x4 cm. at anterior of body of uterus Both normal Normal liver and spleen Normal omentum No immediate comlication Estimate blood loss 800 ml.
- 26. PROGRESS NOTE (12/12/2555) S: Hct 35 vol% O: V/S BP 100/40 mmHg RR 18 /min PR 90/min BT 36.5 c Abd soft, normoactive bowel sound, no tenderness, no active bleeding A+P : Multiple myoma with hypermenorrhea S/P TAH c BSO day 1 : clinical stable Step diet Off IV+Foley Pain control
- 27. PROGRESS NOTE (13/12/2555) S: O: v/s BP 100/50 mmHg RR 18 /min PR 72/min BT 36.8 c Abd soft, normoactive bowel sound, no tenderness, no active bleeding A+P : Multiple myoma with hypermenorrhea S/P TAH c BSO day 2 : clinical stable Observe bleeding Pain control Plan discharge