Downloaded 13 times


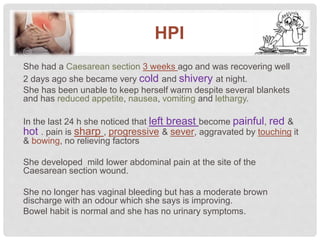












- Mona, a 29-year-old housewife, presented to the ER complaining of fever for 2 days. She had a C-section 3 weeks ago and was recovering well until 2 days ago when she developed fever, reduced appetite, nausea, vomiting and lethargy. She also noticed her left breast became painful, red and hot in the last 24 hours. She has mild lower abdominal pain at the site of her previous C-section incision.



























![1[Shortened Title up to 50 Characters]2Week 9 Assignment.docx](https://cdn.slidesharecdn.com/ss_thumbnails/1shortenedtitleupto50characters2week9assignment-221017192223-b9170776-thumbnail.jpg?width=640&height=640&fit=bounds)
![1[Shortened Title up to 50 Characters]16Week 9 Assignment.docx](https://cdn.slidesharecdn.com/ss_thumbnails/1shortenedtitleupto50characters16week9assignment-221017192230-8773d434-thumbnail.jpg?width=640&height=640&fit=bounds)












![[OBGyne-JRRMMC]--03_15_20252025031525.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/obgynejrrmmc03152025-250507060427-77ad2591-thumbnail.jpg?width=640&height=640&fit=bounds)